

Postoperative external beam radiotherapy for differentiated thyroid cancer: outcomes and morbidity with conformal treatment
- PMID: 19095376
- PMCID: PMC2745400
- DOI: 10.1016/j.ijrobp.2008.09.023
Postoperative external beam radiotherapy for differentiated thyroid cancer: outcomes and morbidity with conformal treatment
Abstract
Purpose: To review institutional outcomes for patients treated for differentiated thyroid cancer with postoperative conformal external beam radiotherapy (EBRT).
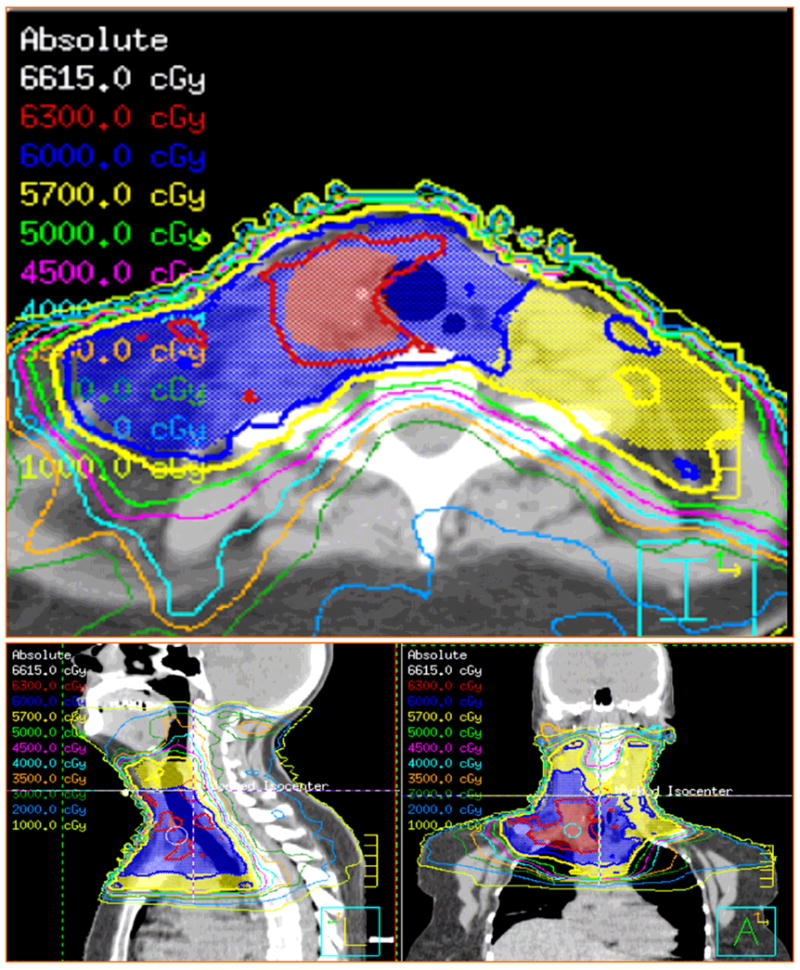
Methods and materials: This is a single-institution retrospective review of 131 consecutive patients with differentiated thyroid cancer who underwent EBRT between January 1996 and December 2005. Histologic diagnoses included 104 papillary, 21 follicular, and six mixed papillary-follicular types. American Joint Committee on Cancer stage distribution was Stage III in 2 patients, Stage IVa-IVc in 128, and not assessable in 1. Thirty-four patients (26%) had high-risk histologic types and 76 (58%) had recurrent disease. Extraglandular disease spread was seen in 126 patients (96%), microscopically positive surgical margins were seen in 62 patients (47%), and gross residual disease was seen in 15 patients (11%). Median EBRT dose was 60 Gy (range, 38-72 Gy). Fifty-seven patients (44%) were treated with intensity-modulated radiotherapy (IMRT) to a median dose of 60 Gy (range, 56-66 Gy). Median follow-up was 38 months (range, 0-134 months).
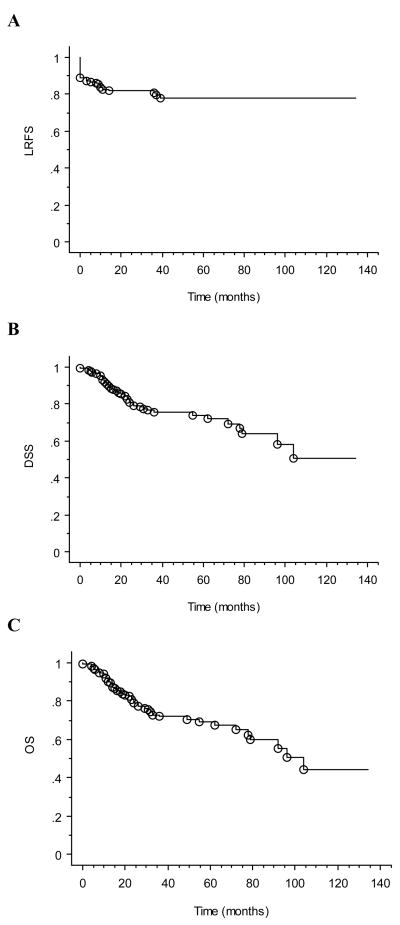
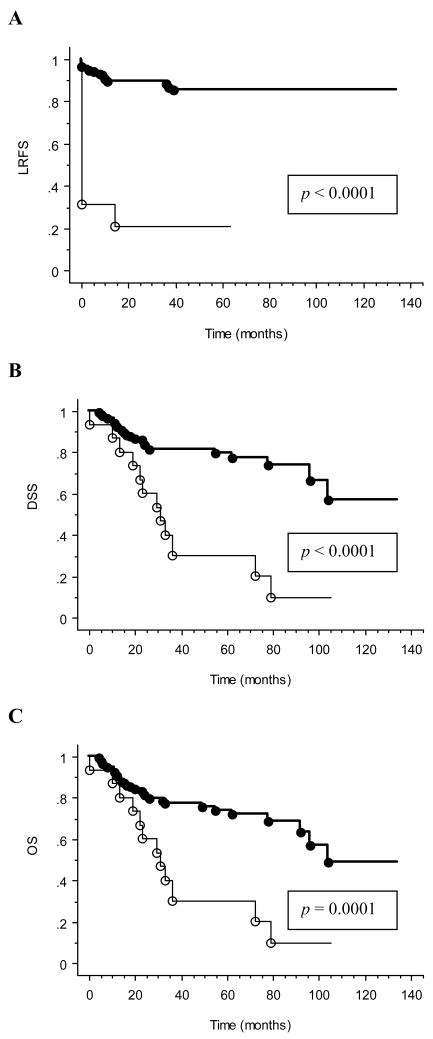
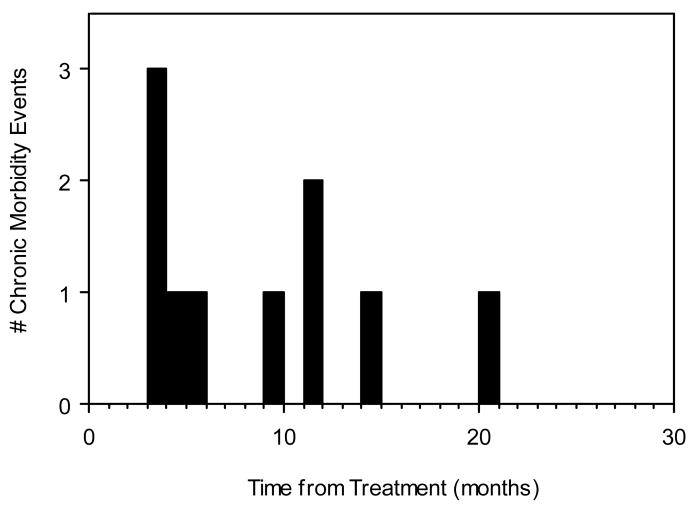
Results: Kaplan-Meier estimates of locoregional relapse-free survival, disease-specific survival, and overall survival at 4 years were 79%, 76%, and 73%, respectively. On multivariate analysis, high-risk histologic features and gross residual disease predicted for inferior locoregional relapse-free survival, whereas high-risk histologic features, M1 disease, and gross residual disease predicted for inferior disease-specific and overall survival. The IMRT did not impact on survival outcomes, but was associated with less frequent severe late morbidity (12% vs. 2%).
Conclusions: Postoperative conformal EBRT provides durable locoregional disease control for patients with high-risk differentiated thyroid cancer if disease is reduced to microscopic burden. Patients with gross disease face significantly worse outcomes. The IMRT may significantly reduce chronic radiation morbidity, but requires additional study.
Conflict of interest statement
Conflicts of Interest: None
Figures
References
-
- Benker G, Olbricht T, Reinwein D, et al. Survival rates in patients with differentiated thyroid carcinoma. Influence of postoperative external radiotherapy. Cancer. 1990;65:1517–1520. - PubMed
-
- Chung CT, Sagerman RH, Ryoo MC, et al. External irradiation for malignant thyroid tumors. Radiology. 1980;136:753–756. - PubMed
-
- Farahati J, Reiners C, Stuschke M, et al. Differentiated thyroid cancer. Impact of adjuvant external radiotherapy in patients with perithyroidal tumor infiltration (stage pT4) Cancer. 1996;77:172–180. - PubMed
-
- Harmer CL. External beam radiotherapy for thyroid cancer. Ann Radiol (Paris) 1977;20:791–800. - PubMed
-
- Phlips P, Hanzen C, Andry G, et al. Postoperative irradiation for thyroid cancer. Eur J Surg Oncol. 1993;19:399–404. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
