

Review
doi: 10.3174/ajnr.A1398.
Epub 2008 Dec 18.
Imaging lesions of the cavernous sinus
Affiliations
- PMID: 19095789
- PMCID: PMC7051469
- DOI: 10.3174/ajnr.A1398
Item in Clipboard
Review
Imaging lesions of the cavernous sinus
AJNR Am J Neuroradiol.
2009 Mar.
Erratum in
- AJNR Am J Neuroradiol. 2009 Aug;30(7):E115
Abstract
Our aim was to review the imaging findings of relatively common lesions involving the cavernous sinus (CS), such as neoplastic, inflammatory, and vascular ones. The most common are neurogenic tumors and cavernoma. Tumors of the nasopharynx, skull base, and sphenoid sinus may extend to the CS as can perineural and hematogenous metastases. Inflammatory, infective, and granulomatous lesions show linear or nodular enhancement of the meninges of the CS but often have nonspecific MR imaging features. In many of these cases, involvement elsewhere suggests the diagnosis. MR imaging is sensitive for detecting vascular lesions such as carotid cavernous fistulas, aneurysms, and thromboses.
Figures
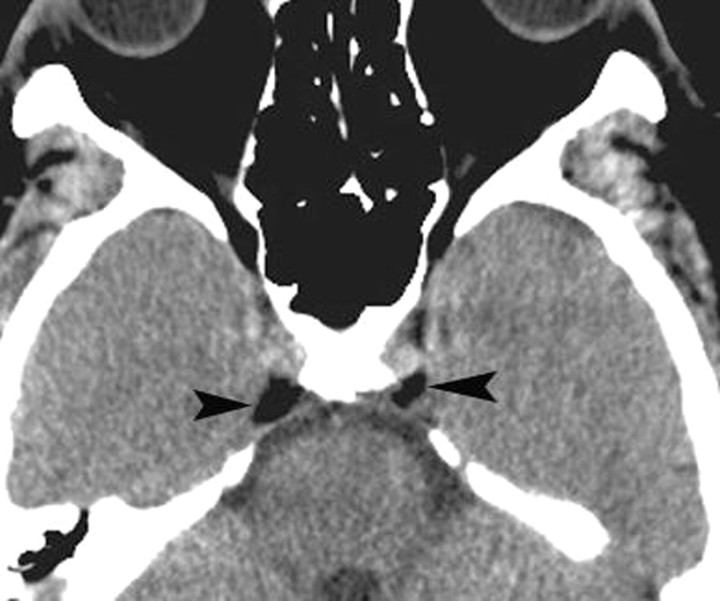
Normal fat deposits. Axial noncontrast CT scan shows normal and incidentally found deposits of fat (arrowheads) in the posterior CSs. These deposits may be seen in obese individuals, those taking corticosteroids, or those with Cushing syndrome. In the absence of these conditions, they have no significance.

Schwannoma. Axial postcontrast T1-weighted image shows a well-defined enhancing mass (arrow) involving the Meckel cave on the right. Although the findings are nonspecific, the most common mass in this location is a schwannoma.
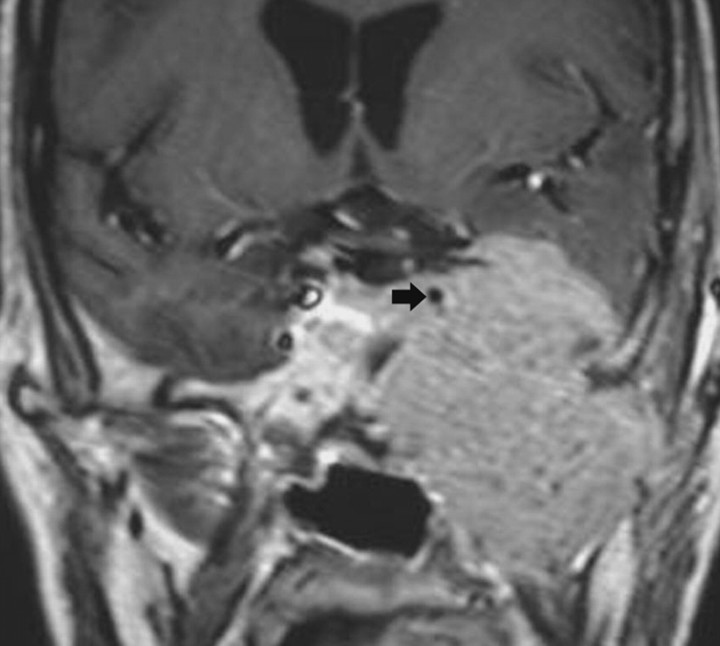
Malignant peripheral nerve sheath tumor. Coronal postcontrast T1-weighted image shows a large aggressive-appearing mass that involves the left CS, surrounds the ICA (arrow), erodes the middle cranial fossa floor, and extends into the infratemporal region.
Cavernous hemangiomas. A, Axial postcontrast T1-weighted image shows a large and homogeneously enhancing mass arising from the lateral wall of the left CS. B, Axial postcontrast T1-weighted image in a different cavernoma, which shows inhomogeneous contrast enhancement but also arises from the lateral wall of the CS, pushing the ICA (arrow) medially. When a mass arises in the lateral wall of a CS, the most important differential diagnosis is that of meningioma versus cavernoma.
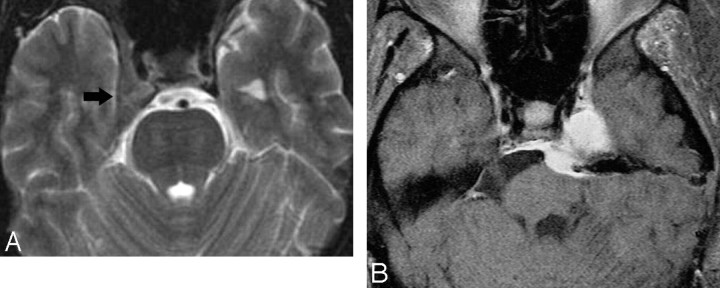
Meningiomas. A, Axial T2-weighted image shows a meningioma (arrow) that is isoattenuated to white matter involving the right CS and extending from the Meckel cave into the superior orbital fissure. B, Axial postcontrast T1-weighted image in a different patient shows the bulk of a homogeneously enhancing mass in the Meckel cave but extending through the porous trigeminus into the prepontine cistern. A schwannoma needs to be considered in the differential diagnosis.
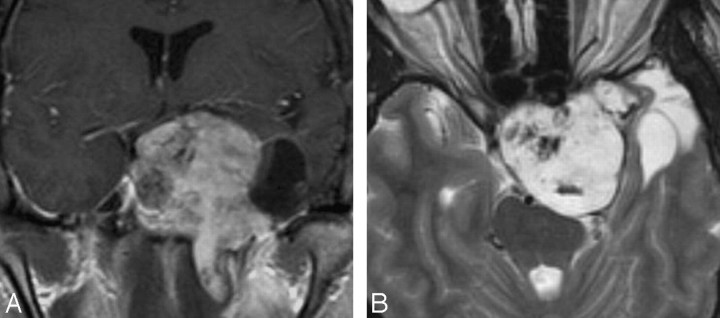
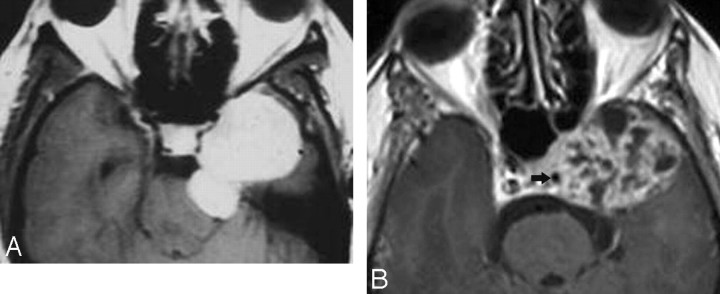
Chondrosarcoma. A, Coronal postcontrast T1-weighted image shows a large inhomogeneous-appearing mass involving the left CS, sella, suprasellar region, ipsilateral middle cranial fossa, and intratemporal region. The mass has a cystic lateral component. B, Axial T2-weighted image shows that the solid portion of the mass is hyperintense, a finding that is typical of chondrosarcoma.
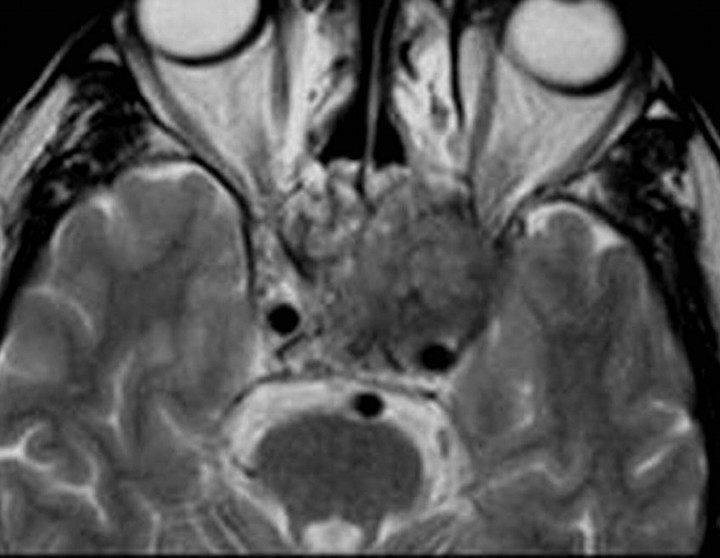
Nasopharyngeal squamous cell carcinoma. Axial T2-weighted image shows a relatively hypointense mass involving the left CS and sella, extending into the posterior ethmoid air cells. Invasive T2 hypointense masses are generally either neoplasias or fungal infections.
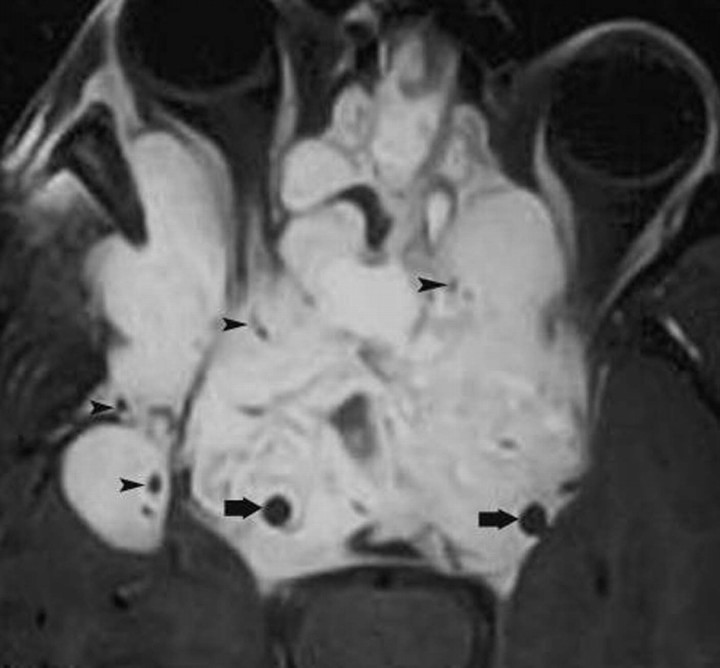
Juvenile angiofibroma. Axial postcontrast T1-weighted image shows a very large tumor involving both CSs and surrounding the ICAs (arrows). The mass extends into the sella, paranasal sinuses, right middle cranial fossa, and both orbits. Note flow voids (arrowheads) due to enlarged blood vessels.
Metastasis. Axial postcontrast T1-weighted image shows an enhancing mass (from primary breast carcinoma) in the right the Meckel cave (arrowhead). In the absence of primary tumor elsewhere, schwannoma needs to be considered in the differential diagnosis.
Perineural tumor spread. A, Coronal postcontrast T1-weighted image shows a thick enhancing third division (arrows) of the right trigeminal nerve in a patient with a small adenoid cystic carcinoma in the nasopharynx. B, Slightly posterior to A, the tumor has invaded the Gasserian ganglion and fills the Meckel cave (arrow).
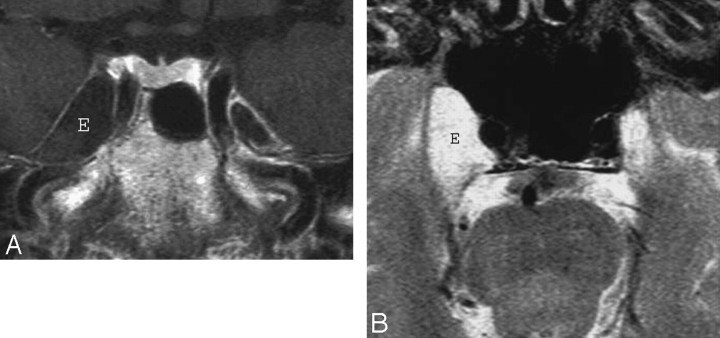
Epidermoid. A, Axial postcontrast T1-weighted image shows a large mass (E) inside the right the Meckel cave. The mass does not enhance and is nearly isointense to CSF. B, Axial T2-weighted image in the same patient shows that the mass (E) is nearly as bright as CSF. Despite the large size of the lesion, clinical symptoms were mild. The differential diagnosis includes an intratemporal meningocele.
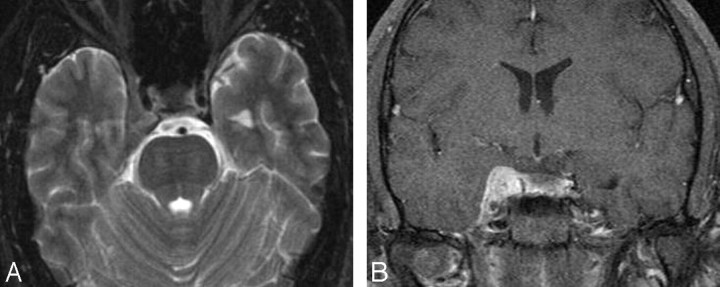
Tolosa-Hunt syndrome. A, Axial T2-weighted image shows hypointense soft tissue throughout the right CS and extending into the superior orbital fissure. B, Coronal postcontrast T1-weighted image shows that the abnormal soft tissue enhances prominently and diffusely and involves the Meckel cave.

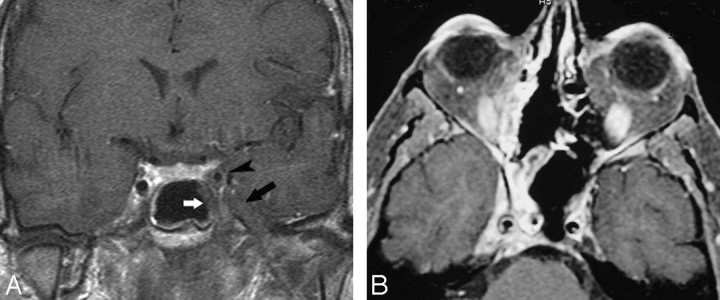
Inflammatory myofibroblastic tumor. A, Axial postcontrast T1-weighted image shows thickening and stranding of the left extraocular muscles more on medial rectus (R) and extension of the process into the ipsilateral CS (arrow). There is prominent enhancement of these muscles and of the retro-orbital fat.

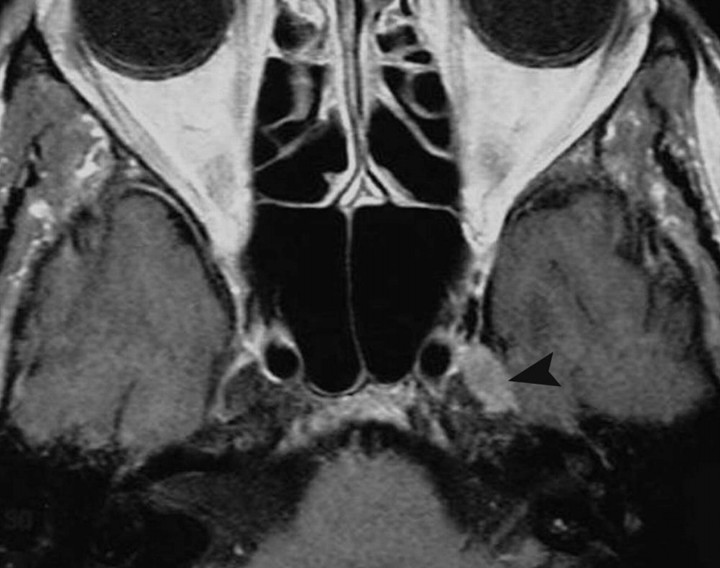
Idiopathic pachymeningitis. Coronal postcontrast T1-weighted image shows nonspecific thickening of the right CS at the level of the foramen ovale. There is perhaps slight thickening of the lateral dural wall of the contralateral CS.
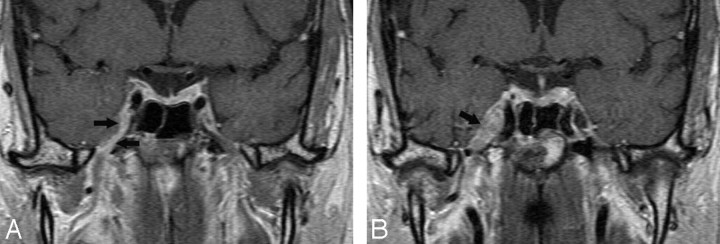
Fungal infection. A, Coronal postcontrast T1-weighted image shows involvement by aspergillosis of the mucosa in the left sphenoid sinus (white arrow), which extends laterally and has resulted in thrombosis of the adjacent CS (black arrow). The intracavernous ICA (arrowhead) is narrowed, and its walls are significantly thickened. B, In a different patient, an axial postcontrast T1-weighted image shows enhancing mucosa in the right sphenoid sinus with enhancing soft tissues in the ipsilateral CS (including the Meckel cave), with narrowing of the ICA and significant thickening of its walls.
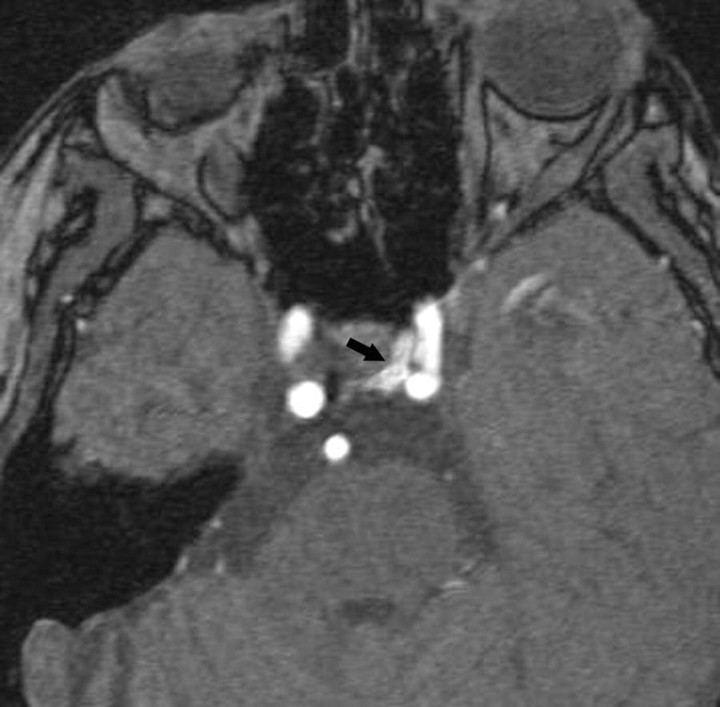
ICA to a CS fistula. Axial source image from an MR angiogram shows flow-related enhancement in the medial (arrow) left CS from a direct-type fistula.
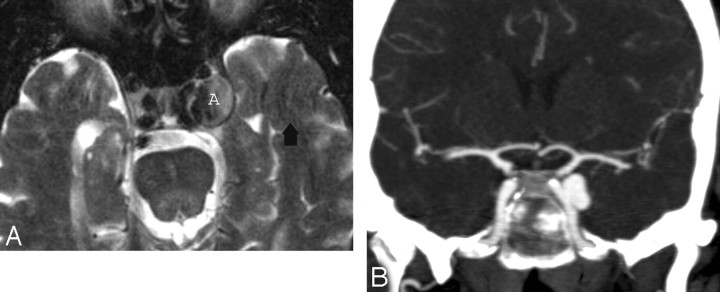
Intracavernous aneurysms. A, Axial T2-weighted image shows a left intracavernous ICA (A) aneurysm. Note flow artifacts (arrow) confirming the pulsatile nature of the lesions. B, Coronal postcontrast maximum-intensity image from a CT angiogram in the same patient shows the left intracavernous aneurysm.
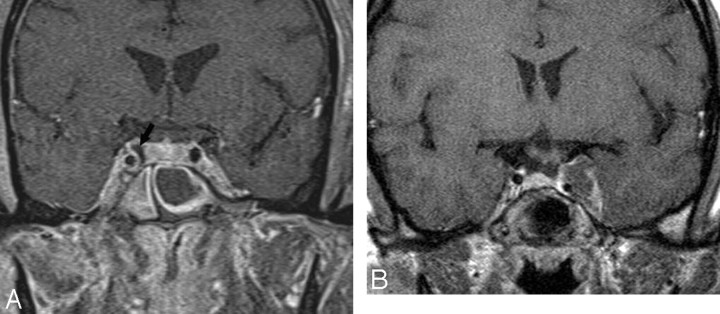
CS thrombosis. A, Coronal postcontrast T1-weighted image shows an enlarged and inhomogeneous-appearing right CS that contains areas of low signal intensity (arrow) compatible with clot. B, Coronal postcontrast T1-weighted image in a different patient shows a large nonenhancing clot expanding the left CS. The ipsilateral ICA is slightly narrowed.
References
-
- Boardman JF, Rothfus WE, Dulai HS. Lesions and pseudolesions of the cavernous sinus and petrous apex. Otolaryngol Clin North Am 2008;41:195–213 - PubMed
-
- Lee JH, Lee HK, Park JK, et al. Cavernous sinus syndrome: clinical features and differential diagnosis with MR imaging. AJR Am J Roentgenol 2003;181:583–90 - PubMed
-
- Castillo M. Imaging of the upper cranial nerves I, III-VIII, and the cavernous sinuses. Magn Reson Imaging Clin North Am 2002;10:415–31 - PubMed
-
- Larson TL. Petrous apex and cavernous sinus: anatomy and pathology. Semin Ultrasound CT MR 1993;14:232–46 - PubMed
-
- Ruscalleda J. Imaging of parasellar lesions. Eur Radiol 2005;15:549–59 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical