

A randomized trial of breakthrough pain during combined spinal-epidural versus epidural labor analgesia in parous women
- PMID: 19095858
- PMCID: PMC2670780
- DOI: 10.1213/ane.0b013e31818f896f
A randomized trial of breakthrough pain during combined spinal-epidural versus epidural labor analgesia in parous women
Abstract
Background: There is controversy regarding the benefits and risks of combined spinal-epidural compared with epidural analgesia (CSE, EPID) for labor analgesia. We hypothesized that CSE would result in fewer patient requests for top-up doses compared to EPID.
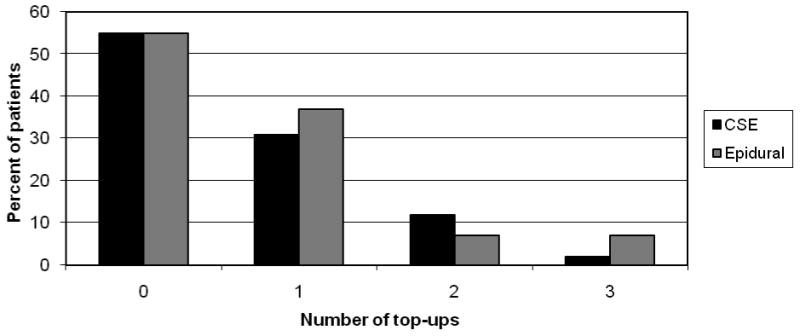
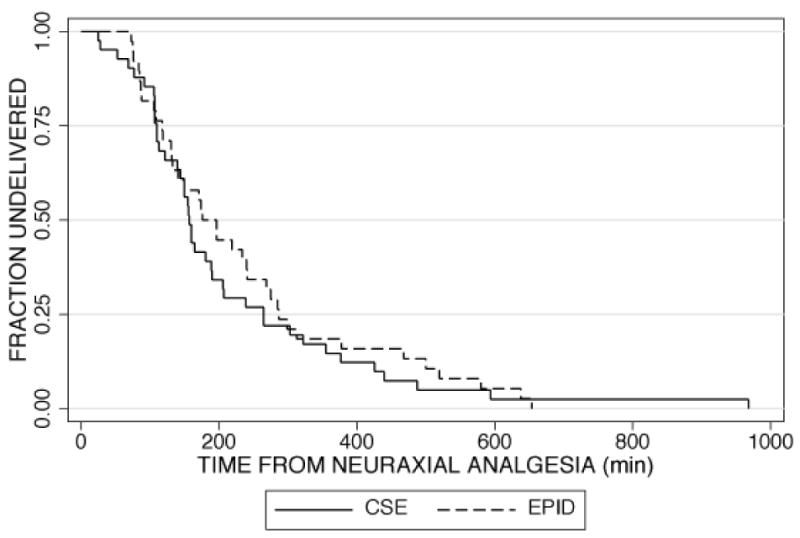
Methods: One-hundred ASA physical status I or II parous women at term in early labor (<5 cm cervical dilation) requesting analgesia were randomized in double-blind fashion to the EPID group (epidural bupivacaine 2.5 mg/mL, 3 mL, followed by bupivacaine 1.25 mg/mL, 10 mL with fentanyl 50 microg) or the CSE group (intrathecal bupivacaine 2.5 mg with fentanyl 25 microg). Both groups received identical infusions of bupivacaine 0.625 mg/mL with fentanyl 2 microg/mL at 12 mL/h. The primary outcome variable was the number of top-up doses requested to treat breakthrough pain.
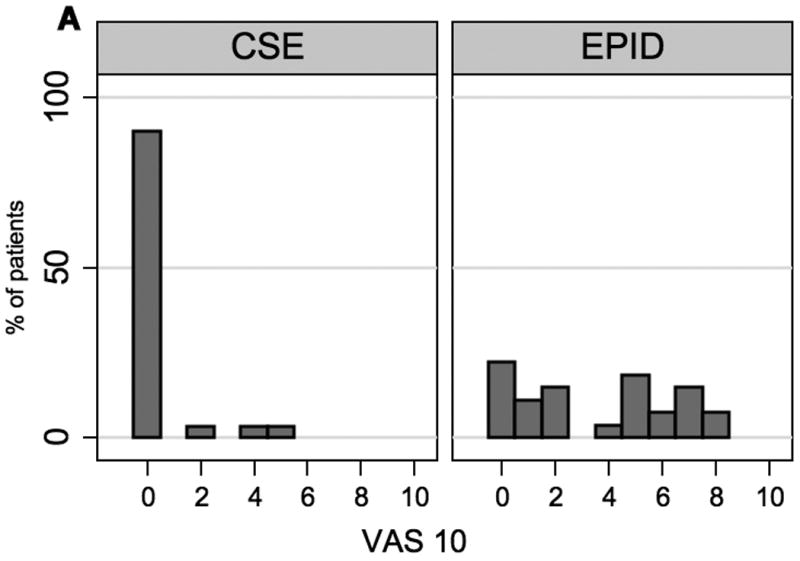
Results: There was no significant difference between the two groups in the percentage of patients requesting top-up doses (44% CSE vs 51% EPID; 95% confidence interval of the difference -28% to +14%) nor in the need for multiple top-up doses (14% CSE vs 15% EPID). Visual analog scale scores were lower in the CSE group compared to the EPID group at 10 min after initiation of analgesia [median 0 cm (0, 0) vs 4 cm (1, 6) respectively, P < 0.001] and at 30 min [0 cm (0, 0) vs 0 cm (0, 1), respectively, P = 0.03].
Conclusions: We did not find a difference in the need for top-up doses in parous patients; however, CSE provided better analgesia in the first 30 min compared to EPID.
Conflict of interest statement
Conflict of Interest: None
References
-
- Simmons S, Cyna A, Dennis A, Hughes D. Combined spinal-epidural versus epidural analgesia in labour. Cochrane Database Syst Rev. 2007;3:CD003401. - PubMed
-
- Tsen LC, Thue B, Datta S, Segal S. Is combined spinal-epidural analgesia associated with more rapid cervical dilation in nulliparous patients when compared with conventional epidural analgesia? Anesthesiology. 1999;91:920–5. - PubMed
-
- Comparative Obstetric Mobile Epidural Trial (COMET) Study Group UK. Effect of low-dose mobile versus traditional epidural techniques on mode of delivery: a randomised controlled trial. Lancet. 2001;358:19–23. - PubMed
-
- Norris MC, Fogel ST, Conway-Long C. Combined spinal-epidural versus epidural labor analgesia. Anesthesiology. 2001;95:913–20. - PubMed
-
- Hess PE, Pratt SD, Lucas TP, Miller CG, Corbett T, Oriol N, Sarna MC. Predictors of breakthrough pain during labor epidural analgesia. Anesth Analg. 2001;93:414–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
