

Detection and localization of intraepithelial neoplasia and invasive carcinoma using fluorescence-reflectance bronchoscopy: an international, multicenter clinical trial
- PMID: 19096306
- PMCID: PMC2845524
- DOI: 10.1097/JTO.0b013e3181914506
Detection and localization of intraepithelial neoplasia and invasive carcinoma using fluorescence-reflectance bronchoscopy: an international, multicenter clinical trial
Erratum in
- J Thorac Oncol. 2009 Apr;4(4):558. Gazdar, Adi [added]
Abstract
Objectives: The primary objective of this study was to evaluate the benefit of using a new fluorescence-reflectance imaging system, Onco-LIFE, for the detection and localization of intraepitheal neoplasia and early invasive squamous cell carcinoma. A secondary objective was to evaluate the potential use of quantitative image analysis with this device for objective classification of abnormal sites.
Design: This study was a prospective, multicenter, comparative, single arm trial. Subjects for this study were aged 45 to 75 years and either current or past smokers of more than 20 pack-years with airflow obstruction, forced expiratory volume in 1 second/forced vital capacity less than 75%, suspected to have lung cancer based on either sputum atypia, abnormal chest roentgenogram/chest computed tomography, or patients with previous curatively treated lung or head and neck cancer within 2 years.
Materials and methods: The primary endpoint of the study was to determine the relative sensitivity of white light bronchoscopy (WLB) plus autofluorescence-reflectance bronchoscopy compared with WLB alone. Bronchoscopy with Onco-LIFE was carried out in two stages. The first stage was performed under white light and mucosal lesions were visually classified. Mucosal lesions were classified using the same scheme in the second stage when viewed with Onco-LIFE in the fluorescence-reflectance mode. All regions classified as suspicious for moderate dysplasia or worse were biopsied, plus at least one nonsuspicious region for control. Specimens were evaluated by the site pathologist and then sent to a reference pathologist, each blinded to the endoscopic findings. Positive lesions were defined as those with moderate/severe dysplasia, carcinoma in situ (CIS), or invasive carcinoma. A positive patient was defined as having at least one lesion of moderate/severe dysplasia, CIS, or invasive carcinoma. Onco-LIFE was also used to quantify the fluorescence-reflectance response (based on the proportion of reflected red light to green fluorescence) for each suspected lesion before biopsy.
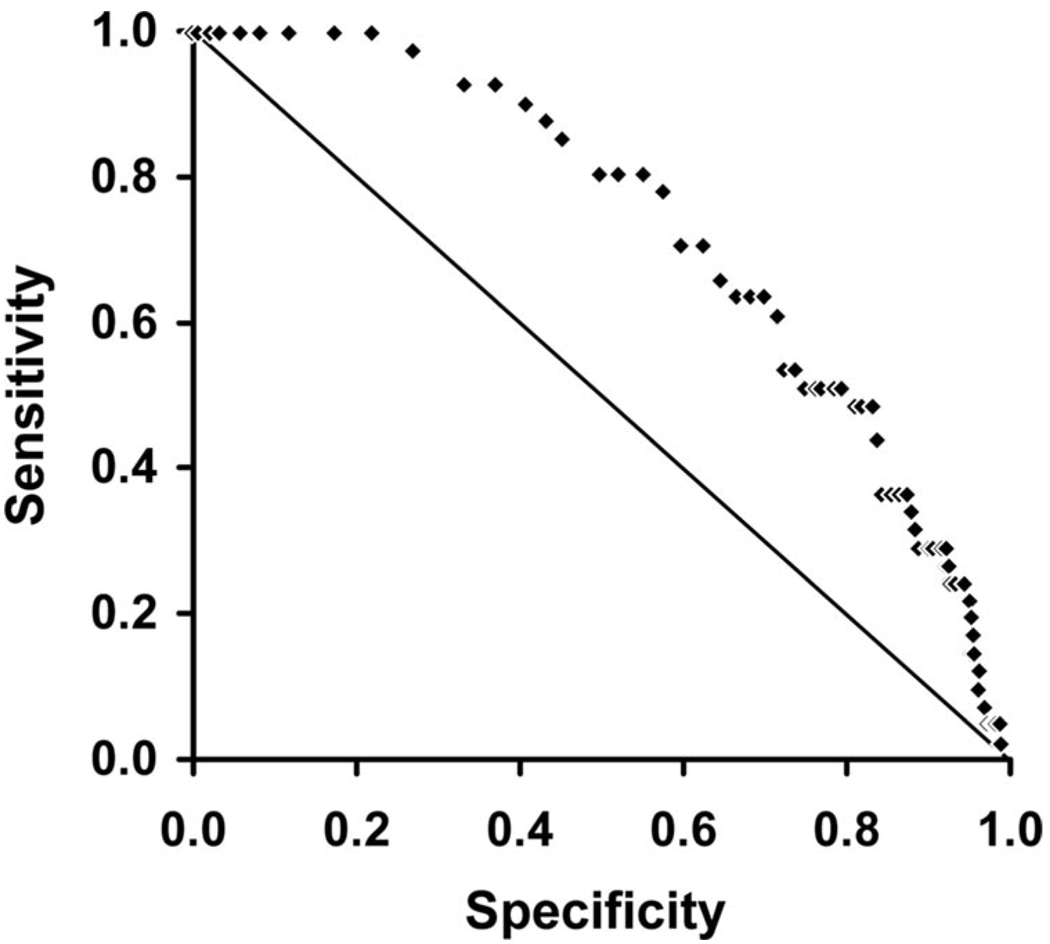
Results: There were 115 men and 55 women with median age of 62 years. Seven hundred seventy-six biopsy specimens were included. Seventy-six were classified as positive (moderate dysplasia or worse) by pathology. The relative sensitivity on a per-lesion basis of WLB + FLB versus WLB was 1.50 (95% confidence interval [CI], 1.26-1.89). The relative sensitivity on a per-patient basis was 1.33 (95% CI, 1.13-1.70). The relative sensitivity to detect intraepithelial neoplasia (moderate/severe dysplasia or CIS) was 4.29 (95% CI, 2.00-16.00) and 3.50 (95% CI, 1.63-12.00) on a per-lesion and per-patient basis, respectively. For a quantified fluorescence reflectance response value of more than or equal to 0.40, a sensitivity and specificity of 51% and 80%, respectively, could be achieved for detection of moderate/severe dsyplasia, CIS, and microinvasive cancer.
Conclusions: Using autofluorescence-reflectance bronchoscopy as an adjunct to WLB with the Onco-LIFE system improves the detection and localization of intraepitheal neoplasia and invasive carcinoma compared with WLB alone. The use of quantitative image analysis to minimize interobserver variation in grading of abnormal sites should be explored further in future prospective clinical trial.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: globocan 2000. Int J Cancer. 2001;94:153–156. - PubMed
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–130. - PubMed
-
- Motta G, Carbone E, Spinelli E, Nahum MA, Testa T, Flocchini GP. Considerations about tumor size as a factor of prognosis in NSCLC. Ann Ital Chir. 1999;70:893–897. - PubMed
-
- Cortese DA, Pairolero PC, Bergstralh EJ, et al. Roentgenographically occult lung cancer: a 10-year experience. J Thorac Cardiovasc Surg. 1983;86:373–380. - PubMed
-
- Bechtel JJ, Petty TL, Saccomanno G. Five year survival and later outcome of patients with X-ray occult lung cancer detected by sputum cytology. Lung Cancer. 2000;30:1–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
