

Arthroscopic femoroplasty in the management of cam-type femoroacetabular impingement
- PMID: 19096902
- PMCID: PMC2635454
- DOI: 10.1007/s11999-008-0659-8
Arthroscopic femoroplasty in the management of cam-type femoroacetabular impingement
Abstract
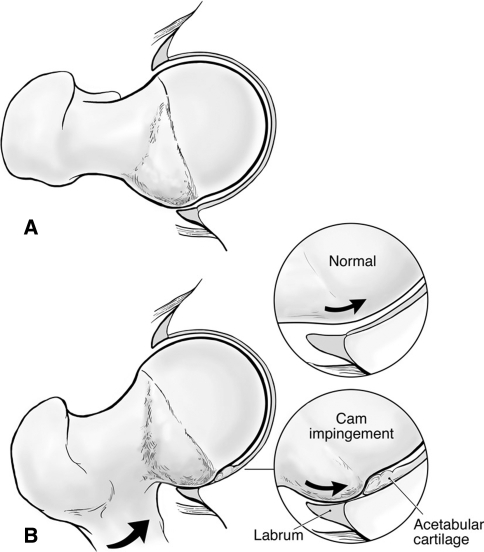
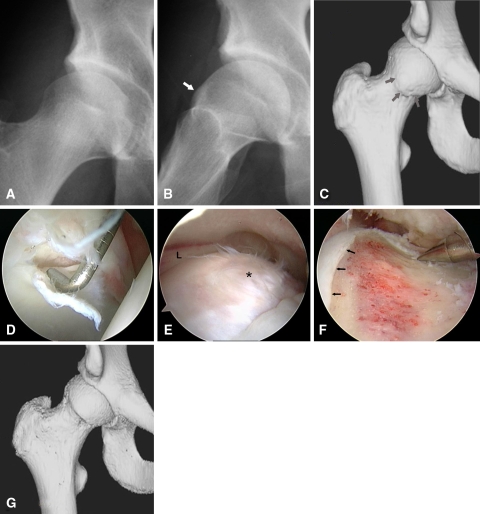
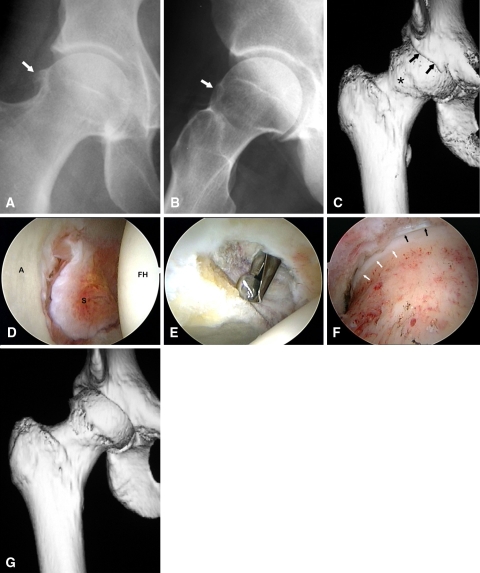
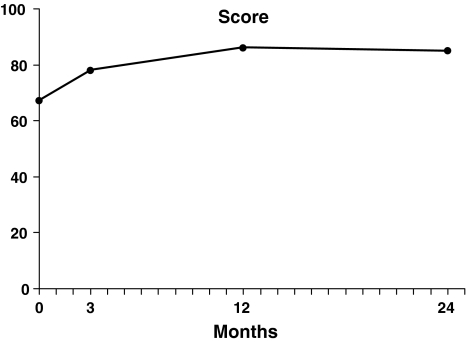
Cam-type femoroacetabular impingement is a recognized cause of intraarticular pathology and secondary osteoarthritis in young adults. Arthroscopy is reportedly useful to treat selected hip abnormalities and has been proposed as a method of correcting underlying impingement. We report the outcomes of arthroscopic management of cam-type femoroacetabular impingement. We prospectively assessed all 200 patients (207 hips) who underwent arthroscopic correction of cam impingement from December 2003 to October 2007, using a modified Harris hip score. The minimum followup was 12 months (mean, 16 months; range, 12-24 months); no patients were lost to followup. The average age was 33 years with 138 men and 62 women. One hundred and fifty-eight patients (163 hips) underwent correction of cam impingement (femoroplasty) alone while 42 patients (44 hips) underwent concomitant correction of pincer impingement. The average increase in Harris hip score was 20 points; 0.5% converted to THA. We had a 1.5% complication rate. The short-term outcomes of arthroscopic treatment of cam-type femoroacetabular impingement are comparable to published reports for open methods with the advantage of a less invasive approach.
Figures
References
-
- Byrd JW. Hip arthroscopy utilizing the supine position. Arthroscopy. 1994;10:275–280. - PubMed
-
- Byrd JW. Hip arthroscopy: evolving frontiers. Op Tech Orthop. 2004;14:58–67. - DOI
-
- Byrd JW, Jones KS. Prospective analysis of hip arthroscopy with two year follow up. Arthroscopy. 2000;16:578–587. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
