

Effect of adding a virtual community (bulletin board) to smokefree.gov: randomized controlled trial
- PMID: 19097974
- PMCID: PMC2630832
- DOI: 10.2196/jmir.1124
Effect of adding a virtual community (bulletin board) to smokefree.gov: randomized controlled trial
Abstract
Background: Demand for online information and help exceeds most other forms of self-help. Web-assisted tobacco interventions (WATIs) offer a potentially low-cost way to reach millions of smokers who wish to quit smoking and to test various forms of online assistance for use/utilization and user satisfaction.
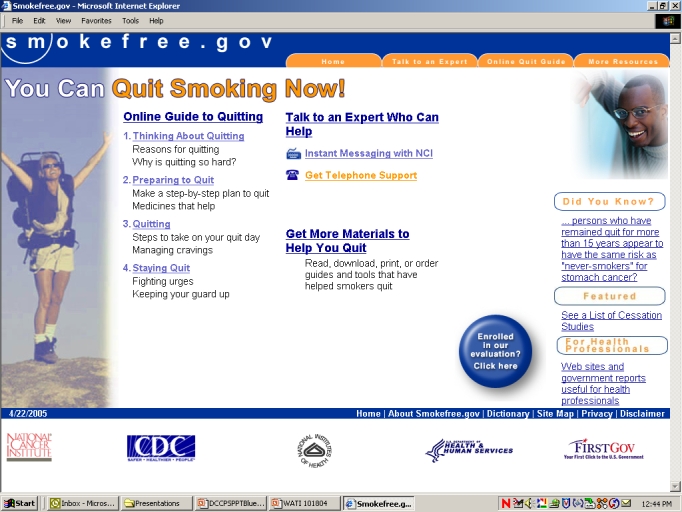
Objectives: Our primary aim was to determine the utilization of and satisfaction with 2 versions of a smoking cessation website (smokefree.gov), one of which included an asynchronous bulletin board (BB condition). A secondary goal was to measure changes in smoking behavior 3 months after enrollment in the study.
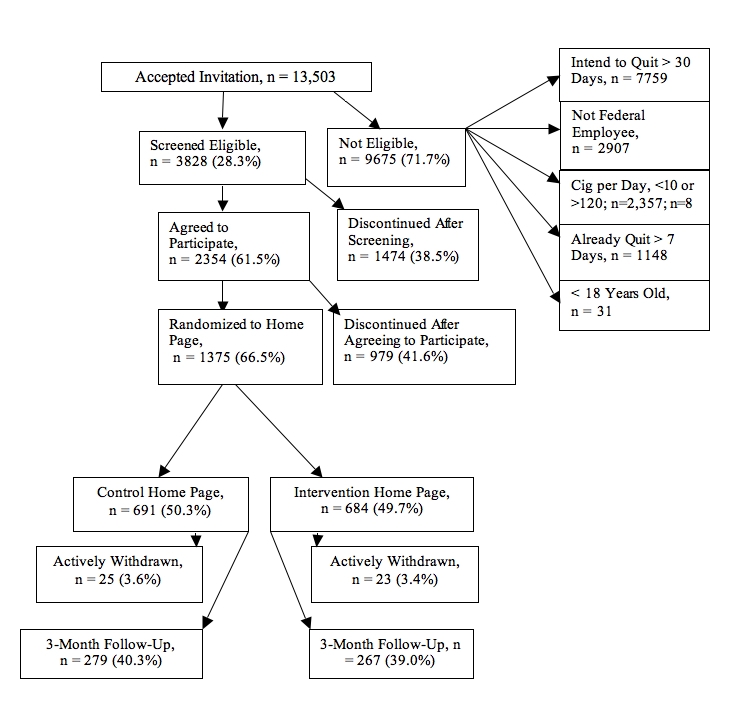
Methods: All participants were adult federal employees or contractors to the federal government who responded to an email and indicated a willingness to quit smoking in 30 days. We randomly assigned participants to either the BB condition or the publicly available version--usual care (UC)--and then assessed the number of minutes of website use and satisfaction with each condition as well as changes in smoking behavior.
Results: Among the 1375 participants, 684 were randomized to the BB intervention, and 691 to the control UC condition. A total of 39.7% returned a follow-up questionnaire after 3 months, with similar rates across the two groups (UC: n=279, 40.3%; BB: n=267, 39.0%). Among those respondents assigned to the BB condition, only 81 participants (11.8%) elected to view the bulletin board or post a message, limiting our ability to analyze the impact of bulletin board use on cessation. Satisfaction with the website was high and did not differ significantly between conditions (UC: 90.2%, BB: 84.9%, P= .08). Utilization, or minutes spent on the website, was significantly longer for the BB than the UC condition (18.0 vs 11.1, P = .01) and was nearly double for those who remained in the study (21.2) than for those lost to follow-up (9.6, P< .001). Similar differences were observed between those who made a serious quit attempt versus those who did not (22.4 vs 10.4, P= .02) and between those with a quit date on or a few days prior to the enrollment date versus those with a later quit date (29.4 vs 12.5, P = .001). There were no statistically significant differences in quit rates between the BB and UC group, both in intent-to-treat analysis (ITT) and in analyzing the adherence subgroup (respondents) only. Combined across the UC and BB groups, 7-day abstinence was 6.8% with ITT and 17.6% using only participants in the follow-up (adherence). For participants who attempted to quit within a few days of study entry (vs 30 days), quit rates were 29.6% (ITT) and 44.4% (adherence).
Conclusions: Quit rates for participants were similar to other WATIs, with the most favorable outcomes demonstrated by smokers ready to quit at the time of enrolling in the trial and smokers using pharmacotherapy. Utilization of the asynchronous bulletin board was lower than expected, and did not have an impact on outcomes (quit rates). Given the demand for credible online resources for smoking cessation, future studies should continue to evaluate use of and satisfaction with Web features and to clarify results in terms of time since last cigarette as well as use of pharmacotherapy.
Trial registration: ClinicalTrials.gov NCT00245076.
Conflict of interest statement
None declared.
Figures
References
-
- Centers for Disease Control and Prevention (CDC) Cigarette smoking among adults-United States, 2006. MMWR Morb Mortal Wkly Rep. 2007 Nov 9;56(44):1157–61. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5644a2.htmmm5644a2 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
