

Thoracic aortic aneurysm: reading the enemy's playbook
- PMID: 19099048
- PMCID: PMC2605304
Thoracic aortic aneurysm: reading the enemy's playbook
Abstract
Background: At the Yale University Center for Thoracic Aortic Disease, we have been using our clinical experience and laboratory investigations to shed light on the pathophysiology of thoracic aortic aneurysm (TAA), the clinical behavior of thoracic aortic aneurysm, and the optimal clinical management.
Materials and methods: The Yale database contains information on 3,000 patients with thoracic aortic aneurysm, with 9,000 patient-years of follow-up and 9,000 imaging studies. Advanced statistical techniques were applied to this information.
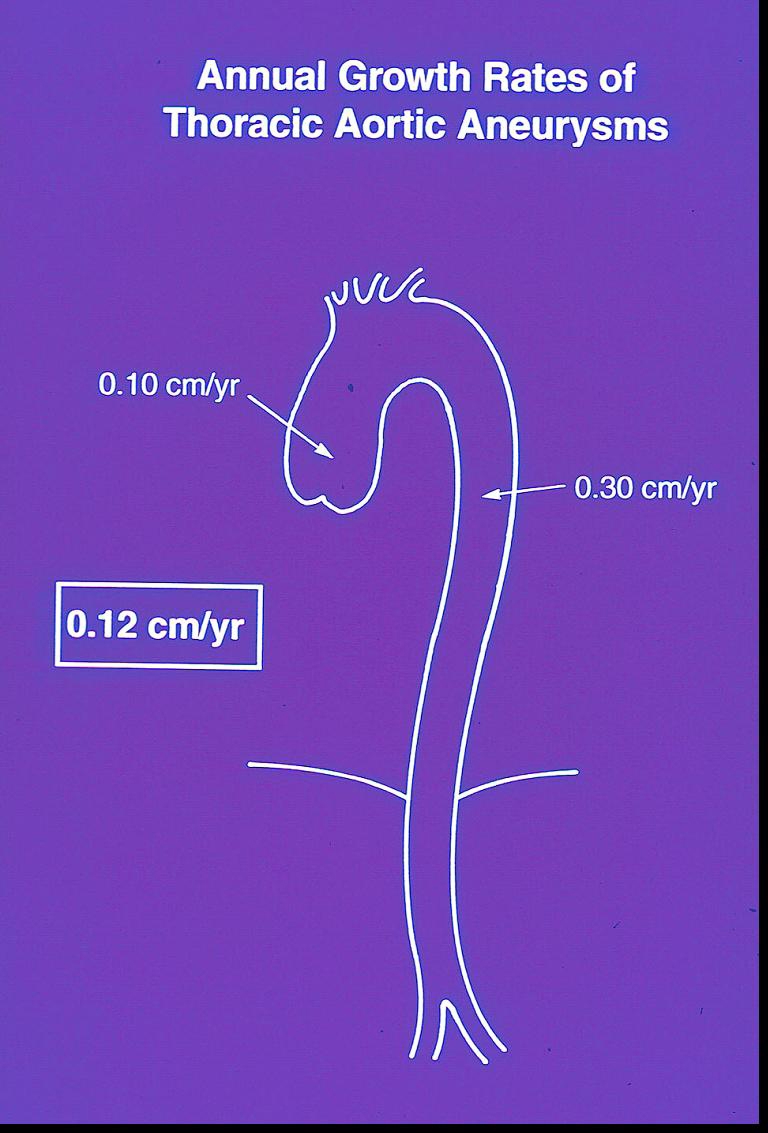
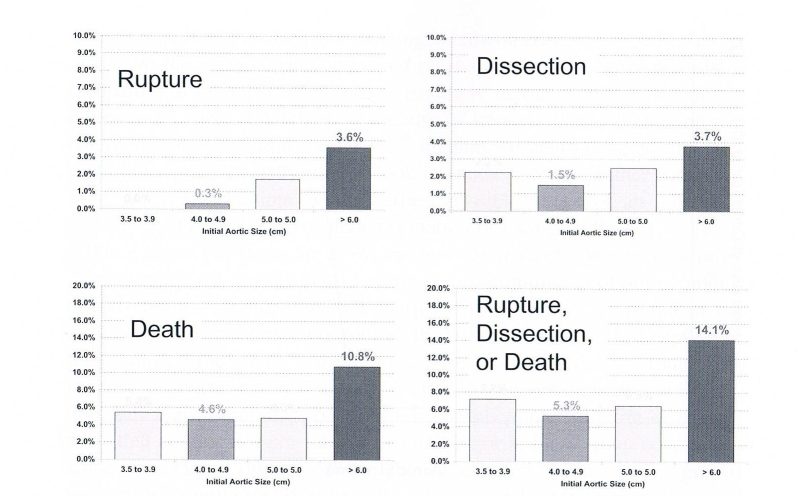
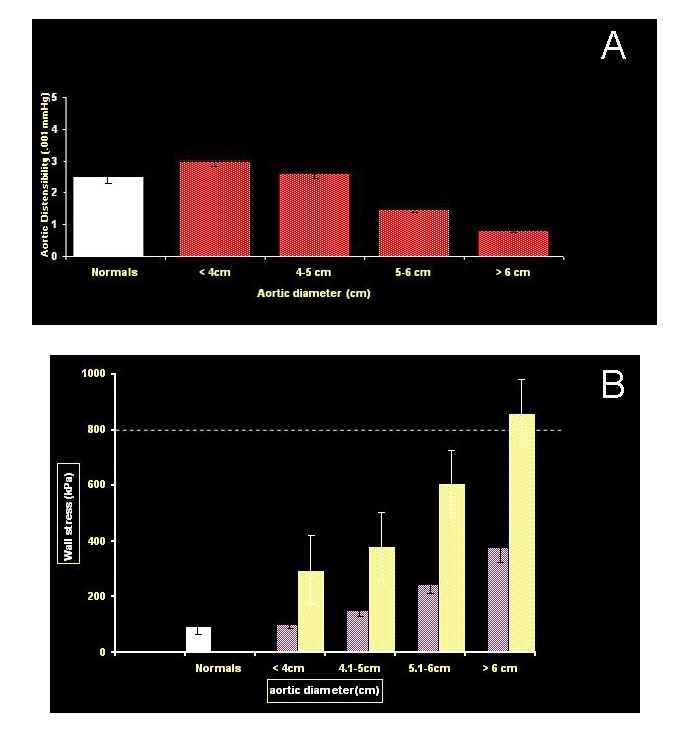
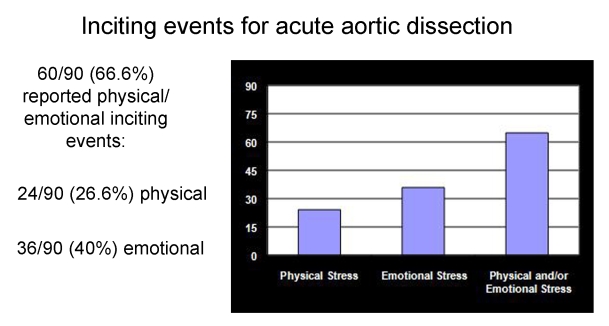
Results: Analysis yielded the following Yale-generated observations: (1) TAA is a genetic disease with a predominantly autosomal dominant mode of inheritance; (2) matrix metalloproteinase (MMP) enzymes are activated in the pathogenesis of TAA; (3) wall tension in TAA approaches the tensile limits of aortic tissue at a diameter of 6 cm; (4) by the time a TAA reaches a clinical diameter of 6 cm, 34 percent of affected patients have suffered dissection or rupture; (5) extreme physical exertion or severe emotion often precipitate acute dissection; and (6) single nucleotide polymorphisms (SNPs) and RNA expression profile changes are being identified that predispose a patient to TAA and can serve as biomarkers for screening for this virulent disease.
Conclusions: The "playbook" of TAA is gradually being read, with the help of scientific investigations, positioning practitioners to combat this lethal disease more effectively than ever before.
Figures










References
-
- Anagnostopoulos CE. Acute Aortic Dissection. Baltimore, MD: University Park Press; 1975.
-
- Rizzo JA, Coady MA, Elefteriades JA. Procedures for estimating growth rates in thoracic aortic aneurysms. J Clin Epidemiol. 1998;51(9):747–754. - PubMed
-
- Koullias GJ, Korkolis DP, Ravichandran P, Psyrri A, Hatzaras I, Elefteriades JA. Tissue microarray detection of matrix metalloproteinases, in diseased tricuspid and bicuspid aortic valves with or without pathology of the ascending aorta. Eur J Cardiothor Surg. 2004;26(6):1098–1103. - PubMed
-
- Morales DLS, Quin JA, Braxton JH, et al. Experimental confirmation of effectiveness of fenestration in acute aortic dissection. Ann Thorac Surg. 1998;66:1679–1683. - PubMed
-
- Coady MA, Davies RB, Roberts M, et al. Familial patterns of thoracic aortic aneurysm. Arch Surg. 1999;134:361–367. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources