

Towards comprehensive assessment of mitral regurgitation using cardiovascular magnetic resonance
- PMID: 19102740
- PMCID: PMC2621154
- DOI: 10.1186/1532-429X-10-61
Towards comprehensive assessment of mitral regurgitation using cardiovascular magnetic resonance
Abstract
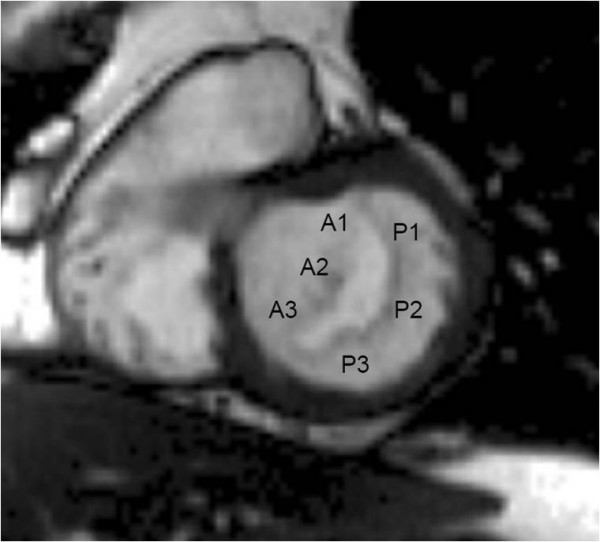
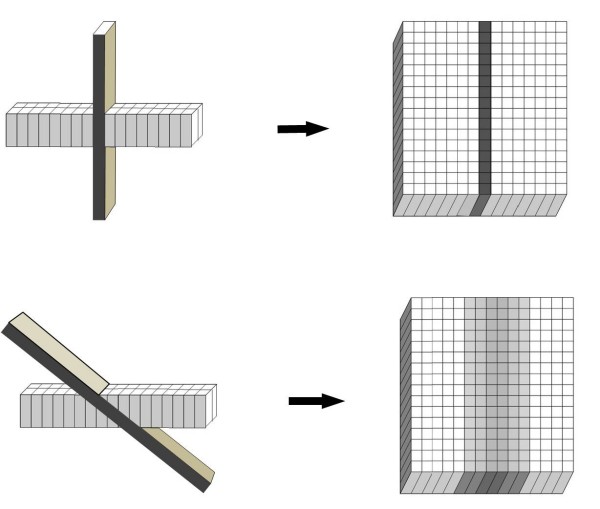
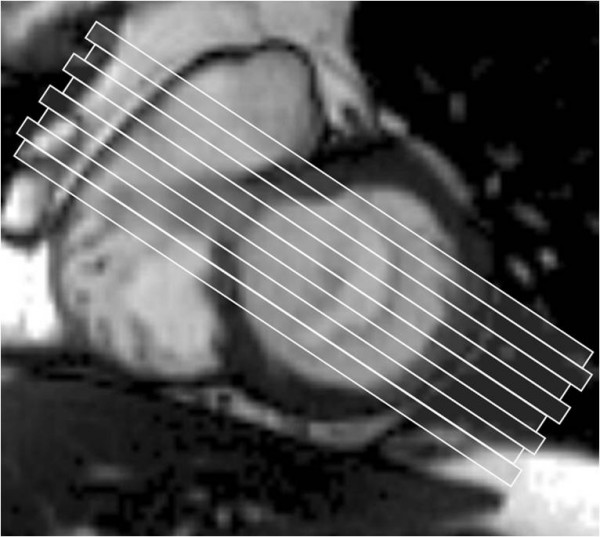
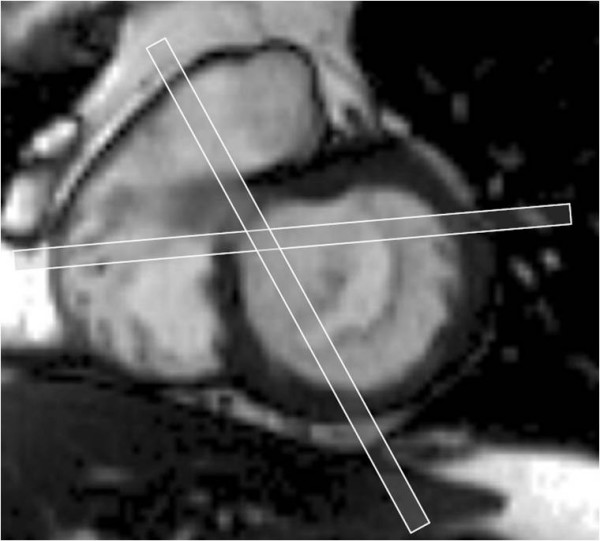
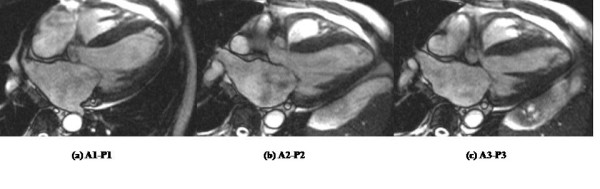
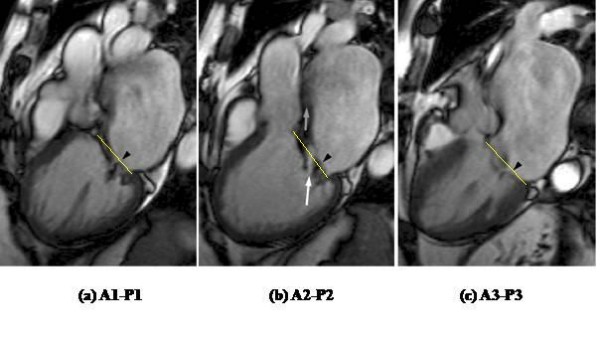
Cardiovascular magnetic resonance (CMR) is increasingly used to assess patients with mitral regurgitation. Its advantages include quantitative determination of ventricular volumes and function and the mitral regurgitant fraction, and in ischemic mitral regurgitation, regional myocardial function and viability. In addition to these, identification of leaflet prolapse or restriction is necessary when valve repair is contemplated. We describe a systematic approach to the evaluation of mitral regurgitation using CMR which we have used in 149 patients with varying etiologies and severity of regurgitation over a 15 month period. Following standard ventricular cine acquisitions, including 2, 3 and 4 chamber long axis views and a short axis stack for biventricular function, we image movements of all parts of the mitral leaflets using a contiguous stack of oblique long axis cines aligned orthogonal to the central part of the line of coaptation. The 8-10 slices in the stack, orientated approximately parallel to a 3-chamber view, are acquired sequentially from the superior (antero-lateral) mitral commissure to the inferior (postero-medial) commissure, visualising each apposing pair of anterior and posterior leaflet scallops in turn (A1-P1, A2-P2 and A3-P3). We use balanced steady state free precession imaging at 1.5 Tesla, slice thickness 5 mm, with no inter-slice gaps. Where the para-commissural coaptation lines curve relative to the central region, two further oblique cines are acquired orthogonal to the line of coaptation adjacent to each commissure. To quantify mitral regurgitation, we use phase contrast velocity mapping to measure aortic outflow, subtracting this from the left ventricular stroke volume to calculate the mitral regurgitant volume which, when divided by the left ventricular stroke volume, gives the mitral regurgitant fraction. In patients with ischemic mitral regurgitation, we further assess regional left ventricular function and, with late gadolinium enhancement, myocardial viability. Comprehensive assessment of mitral regurgitation using CMR is feasible and enables determination of mitral regurgitation severity, associated leaflet prolapse or restriction, ventricular function and viability in a single examination and is now routinely performed at our centre. The mitral valve stack of images is particularly useful and easy to acquire.
Figures
References
-
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons. Bonow RO, Carabello BA, Kanu C, de Leon AC, Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation. 2006;114:e84–231. doi: 10.1161/CIRCULATIONAHA.106.176857. - DOI - PubMed
-
- Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90:29–34. doi: 10.1016/S0002-9149(02)02381-0. - DOI - PubMed
-
- Gelfand EV, Hughes S, Hauser TM, Yeon SB, Goepfert L, Kissinger KV, Rofsky NM, Manning WJ. Severity of mitral and aortic regurgitation as assessed by cardiovascular magnetic resonance: optimizing correlation with doppler echocardiography. J Cardiovasc Mag Res. 2006;8:503–507. doi: 10.1080/10976640600604856. - DOI - PubMed
