

In-reach specialist nursing teams for residential care homes: uptake of services, impact on care provision and cost-effectiveness
- PMID: 19102743
- PMCID: PMC2627849
- DOI: 10.1186/1472-6963-8-269
In-reach specialist nursing teams for residential care homes: uptake of services, impact on care provision and cost-effectiveness
Abstract
Background: A joint NHS-Local Authority initiative in England designed to provide a dedicated nursing and physiotherapy in-reach team (IRT) to four residential care homes has been evaluated. The IRT supported 131 residents and maintained 15 'virtual' beds for specialist nursing in these care homes.
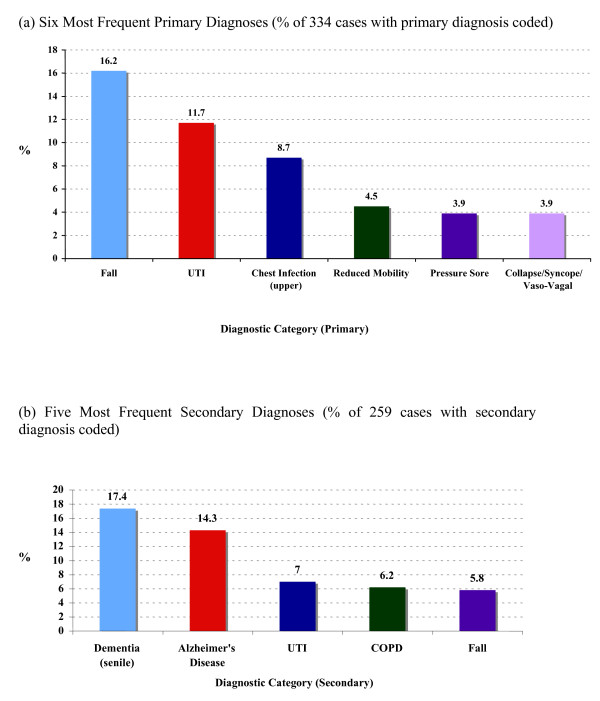
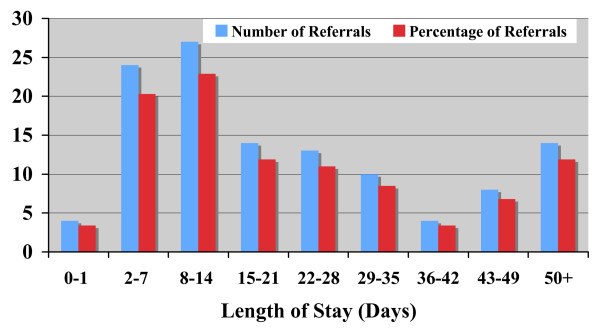
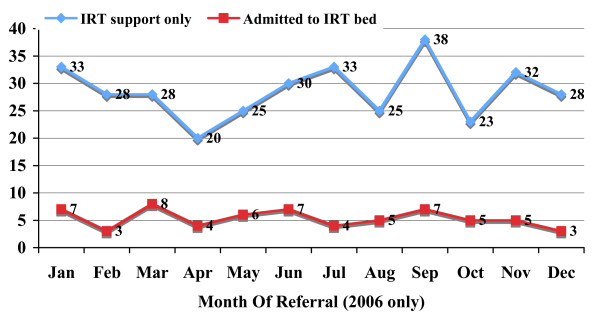
Methods: Data captured prospectively (July 2005 to June 2007) included: numbers of referrals; reason for referral; outcome (e.g. admission to IRT bed, short-term IRT support); length of stay in IRT; prevented hospital admissions; early hospital discharges; avoided nursing home transfers; and detection of unrecognised illnesses. An economic analysis was undertaken.
Results: 733 referrals were made during the 2 years (range 0.5 to 13.0 per resident per annum) resulting in a total of 6,528 visits. Two thirds of referrals aimed at maintaining the resident's independence in the care home. According to expert panel assessment, 197 hospital admissions were averted over the period; 20 early discharges facilitated; and 28 resident transfers to a nursing home prevented. Detection of previously unrecognised illnesses accounted for a high number of visits. Investment in IRT equalled 44.38 pounds per resident per week. Savings through reduced hospital admissions, early discharges, delayed transfers to nursing homes, and identification of previously unrecognised illnesses are conservatively estimated to produce a final reduction in care cost of 6.33 pounds per resident per week. A sensitivity analysis indicates this figure might range from a weekly overall saving of 36.90 pounds per resident to a 'worst case' estimate of 2.70 pounds extra expenditure per resident per week.Evaluation early in implementation may underestimate some cost-saving activities and greater savings may emerge over a longer time period. Similarly, IRT costs may reduce over time due to the potential for refinement of team without major loss in effectiveness.
Conclusion: Introduction of a specialist nursing in-reach team for residential homes is at least cost neutral and, in all probability, cost saving. Further benefits include development of new skills in the care home workforce and enhanced quality of care. Residents are enabled to stay in familiar surroundings rather than unnecessarily spending time in hospital or being transferred to a higher dependency nursing home setting.
Figures
Similar articles
-
Reducing unplanned hospital admissions from care homes: a systematic review.Health Soc Care Deliv Res. 2023 Oct;11(18):1-130. doi: 10.3310/KLPW6338. Health Soc Care Deliv Res. 2023. PMID: 37916580
-
Evaluating mental health decision units in acute care pathways (DECISION): a quasi-experimental, qualitative and health economic evaluation.Health Soc Care Deliv Res. 2023 Dec;11(25):1-221. doi: 10.3310/PBSM2274. Health Soc Care Deliv Res. 2023. PMID: 38149657
-
Reducing potentially preventable hospital transfers: results from a thirty nursing home collaborative.J Am Med Dir Assoc. 2012 Sep;13(7):651-6. doi: 10.1016/j.jamda.2012.06.011. Epub 2012 Jul 25. J Am Med Dir Assoc. 2012. PMID: 22835484
-
Dementia Care Mapping™ to reduce agitation in care home residents with dementia: the EPIC cluster RCT.Health Technol Assess. 2020 Mar;24(16):1-172. doi: 10.3310/hta24160. Health Technol Assess. 2020. PMID: 32216870 Free PMC article. Clinical Trial.
-
A randomized trial of comprehensive geriatric assessment and home intervention in the care of hospitalized patients.Age Ageing. 1999 Oct;28(6):543-50. doi: 10.1093/ageing/28.6.543. Age Ageing. 1999. PMID: 10604506 Clinical Trial.
Cited by
-
A systematic review of integrated working between care homes and health care services.BMC Health Serv Res. 2011 Nov 24;11:320. doi: 10.1186/1472-6963-11-320. BMC Health Serv Res. 2011. PMID: 22115126 Free PMC article.
-
Effective health care for older people living and dying in care homes: a realist review.BMC Health Serv Res. 2016 Jul 16;16:269. doi: 10.1186/s12913-016-1493-4. BMC Health Serv Res. 2016. PMID: 27422733 Free PMC article. Review.
-
Appropriateness of unscheduled hospital admissions from care homes.Clin Med (Lond). 2016 Apr;16(2):103-8. doi: 10.7861/clinmedicine.16-2-103. Clin Med (Lond). 2016. PMID: 27037376 Free PMC article.
-
Relationships, expertise, incentives, and governance: supporting care home residents' access to health care. An interview study from England.J Am Med Dir Assoc. 2015 May 1;16(5):427-32. doi: 10.1016/j.jamda.2015.01.072. Epub 2015 Feb 14. J Am Med Dir Assoc. 2015. PMID: 25687930 Free PMC article.
-
Understanding Pathways into Care-homes using Data (UnPiCD study): a two-part model to estimate inpatient and care-home costs using national linked health and social care data.BMC Health Serv Res. 2024 Mar 5;24(1):281. doi: 10.1186/s12913-024-10675-z. BMC Health Serv Res. 2024. PMID: 38443919 Free PMC article.
References
-
- Royal Commission on Long Term Care With respect to old age: Long term care – rights and responsibilities London. 1999.
-
- Foresight Ageing Population Panel The age shift – Priorities for action London. 1999.
-
- Audit Commission Services for older people London. 2000.
-
- Audit Commission The way to go home: Rehabilitation and remedial services for older people London. 2000.
-
- Wanless D, Fernandez J, Poole T, Beesley L, Henwood M, Moscone F. Securing Good Care for Older People: Taking a long-term view London. 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
