

Body mass index and vigorous physical activity and the risk of heart failure among men
- PMID: 19103991
- PMCID: PMC2727738
- DOI: 10.1161/CIRCULATIONAHA.108.807289
Body mass index and vigorous physical activity and the risk of heart failure among men
Abstract
Background: Elevated body mass index (BMI; weight in kilograms divided by height in meters squared) in the obese range (> or =30 kg/m(2)) is associated with an excess risk of heart failure (HF). However, the impact of overweight or preobese (BMI, 25 to 29.9 kg/m(2)) status and physical activity on HF risk is unclear.
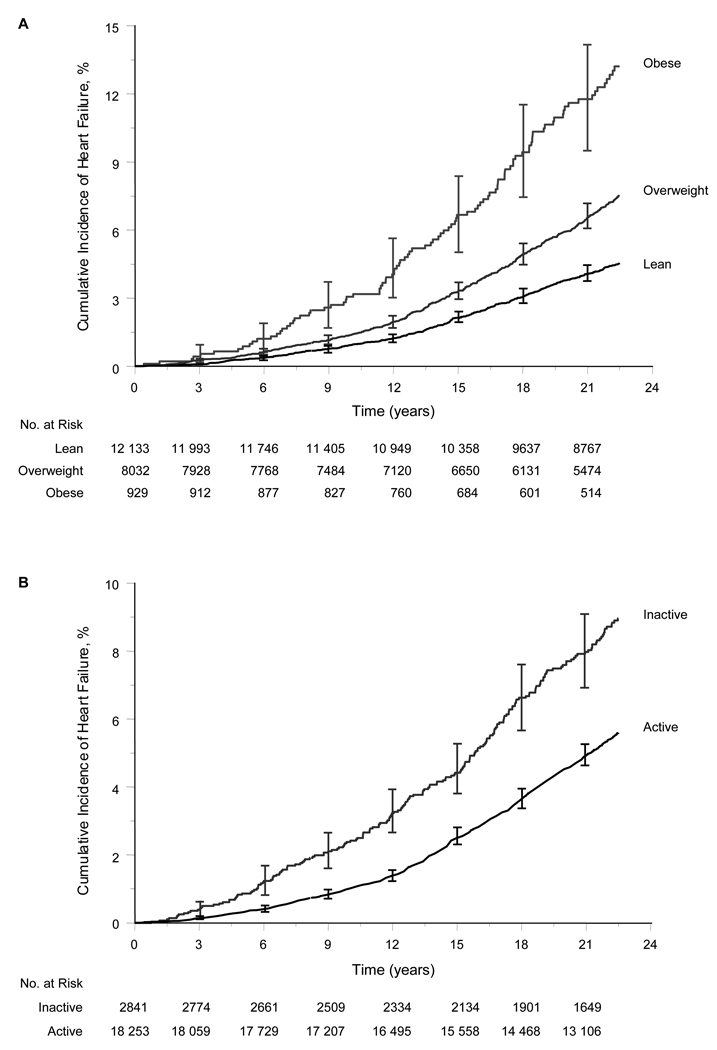
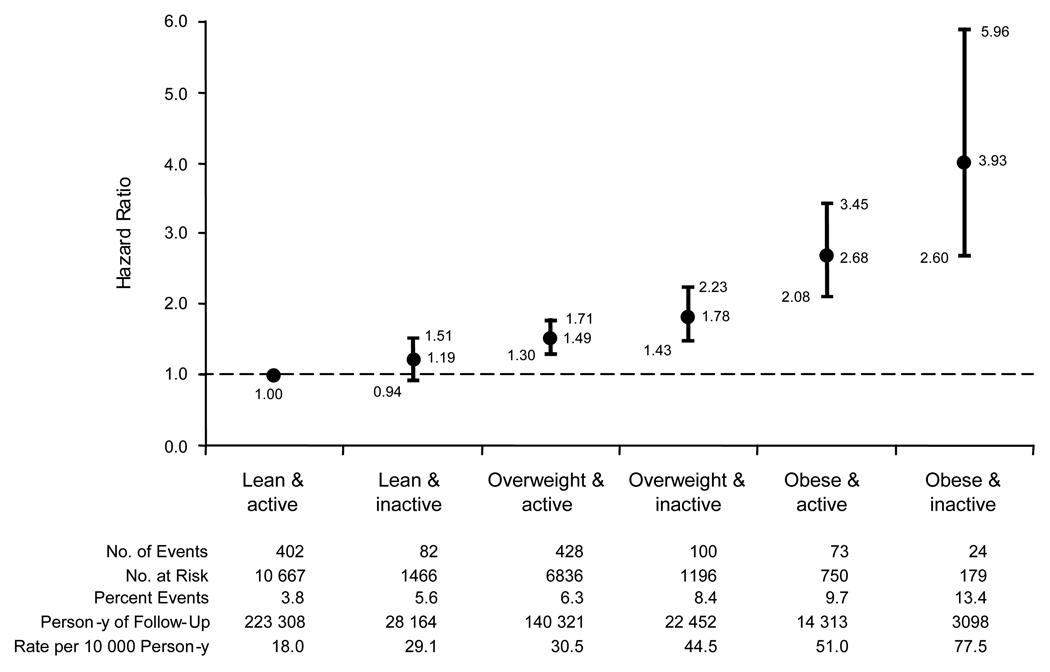
Methods and results: In a prospective cohort of 21,094 men (mean age, 53 years) without known coronary heart disease at baseline in the Physicians' Health Study, we examined the individual and combined effects of BMI and vigorous physical activity (exercise to the point of breaking a sweat) on HF incidence from 1982 to 2007. We evaluated BMI as both a continuous (per 1-kg/m(2) increment) and a categorical (lean, <25 kg/m(2); overweight, 25 to 29.9 kg/m(2); and obese, > or =30 kg/m(2)) variable; we evaluated vigorous physical activity primarily as a dichotomous variable (inactive [rarely/never] versus active [> or =1 to 3 times a month]). During follow-up (mean, 20.5 years), 1109 participants developed new-onset HF. In multivariable analyses, every 1-kg/m(2) increase in BMI was associated with an 11% (95% confidence interval [CI], 9 to 13) increase in HF risk. Compared with lean participants, overweight participants had a 49% (95% CI, 32 to 69) and obese participants had a 180% (95% CI, 124 to 250) increase in HF risk. Vigorous physical activity conferred an 18% (95% CI, 4 to 30) decrease in HF risk. No interaction was found between BMI and vigorous physical activity and HF risk (P=0.96). Lean active men had the lowest and obese inactive men had the highest risk of HF. Compared with lean active men, the hazard ratios were 1.19 (95% CI, 0.94 to 1.51), 1.49 (95% CI, 1.30 to 1.71), 1.78 (95% CI, 1.43 to 2.23), 2.68 (95% CI, 2.08 to 3.45), and 3.93 (95% CI, 2.60 to 5.96) in lean inactive, overweight active, overweight inactive, obese active, and obese inactive men, respectively.
Conclusions: In this cohort of men, elevated BMI, even in the preobese range, was associated with an increased risk of HF, and vigorous physical activity was associated with a decreased risk. Public health measures to curtail excess weight, to maintain optimal weight, and to promote physical activity may limit the scourge of HF.
Conflict of interest statement
None
Figures
Comment in
-
Letter by Hansel and Simon regarding article, "Body mass index and vigorous physical activity and the risk of heart failure among men".Circulation. 2009 Sep 15;120(11):e90; author reply e91. doi: 10.1161/CIRCULATIONAHA.109.862532. Circulation. 2009. PMID: 19752348 No abstract available.
References
-
- Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. National Institutes of Health; 1998. Sep, Report No.: NIH Publication No. 98–4083. - PubMed
-
- WHO Technical Report. Geneva, Switzerland: World Health Organization; 2000. Obesity: Preventing and Managing the Global Epidemic. - PubMed
-
- The World Health Report 2002: Reducing risks, promoting healthy life. Geneva, Switzerland: 2002. - PubMed
-
- United States overweight and obesity prevalence estimates for 2006 and physical activity prevalence estimates for 2007. Atlanta, Ga: Department of Health and Human Services, Behavioral Risk Factor Surveillance System, Centers for Disease Control and Prevention; [Accessed October 15, 2008]. Available at http://apps.nccd.cdc.gov/brfss/list.asp?cat=OB&yr=2006&qkey=4409&state=All and http://apps.nccd.cdc.gov/PASurveillance/StateSumV.asp.
-
- Global overweight and obesity estimates for 2005 and physical inactivity: a global public health problem. Geneva, Switzerland: World Health Organization; [Accessed October 15, 2008]. Available at http://www.who.int/mediacentre/factsheets/fs311/en/print.html and http://www.who.int/dietphysicalactivity/factsheet_inactivity/en/print.html.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
