

Myocardial adeno-associated virus serotype 6-betaARKct gene therapy improves cardiac function and normalizes the neurohormonal axis in chronic heart failure
- PMID: 19103992
- PMCID: PMC2647661
- DOI: 10.1161/CIRCULATIONAHA.108.803999
Myocardial adeno-associated virus serotype 6-betaARKct gene therapy improves cardiac function and normalizes the neurohormonal axis in chronic heart failure
Abstract
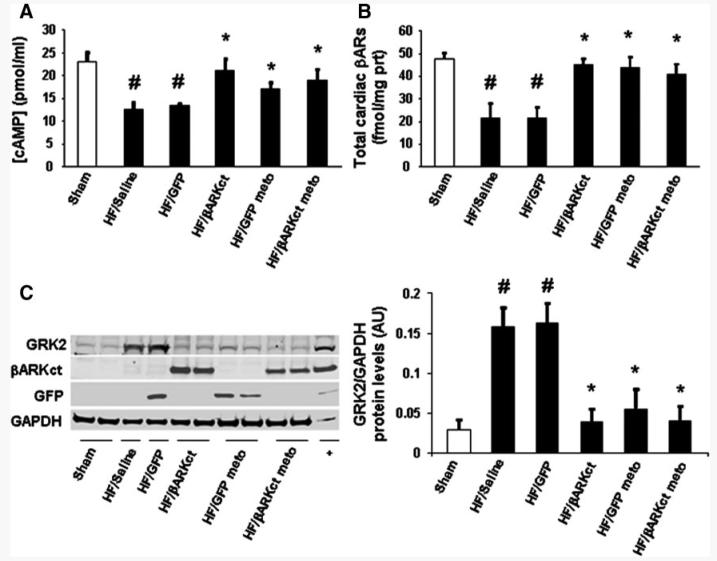
Background: The upregulation of G protein-coupled receptor kinase 2 in failing myocardium appears to contribute to dysfunctional beta-adrenergic receptor (betaAR) signaling and cardiac function. The peptide betaARKct, which can inhibit the activation of G protein-coupled receptor kinase 2 and improve betaAR signaling, has been shown in transgenic models and short-term gene transfer experiments to rescue heart failure (HF). This study was designed to evaluate long-term betaARKct expression in HF with the use of stable myocardial gene delivery with adeno-associated virus serotype 6 (AAV6).
Methods and results: In HF rats, we delivered betaARKct or green fluorescent protein as a control via AAV6-mediated direct intramyocardial injection. We also treated groups with concurrent administration of the beta-blocker metoprolol. We found robust and long-term transgene expression in the left ventricle at least 12 weeks after delivery. betaARKct significantly improved cardiac contractility and reversed left ventricular remodeling, which was accompanied by a normalization of the neurohormonal (catecholamines and aldosterone) status of the chronic HF animals, including normalization of cardiac betaAR signaling. Addition of metoprolol neither enhanced nor decreased betaARKct-mediated beneficial effects, although metoprolol alone, despite not improving contractility, prevented further deterioration of the left ventricle.
Conclusions: Long-term cardiac AAV6-betaARKct gene therapy in HF results in sustained improvement of global cardiac function and reversal of remodeling at least in part as a result of a normalization of the neurohormonal signaling axis. In addition, betaARKct alone improves outcomes more than a beta-blocker alone, whereas both treatments are compatible. These findings show that betaARKct gene therapy can be of long-term therapeutic value in HF.
Figures





References
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397–1402. - PubMed
-
- Harnad E, Mather PJ, Srinivasan S, Rubin S, Whellan DJ, Feldman AM. Pharmacologic therapy of chronic heart failure. Am J Cardiovasc Drugs. 2007;7:235–248. - PubMed
-
- Rockman HA, Koch WJ, Lefkowitz RJ. Seven-transmembrane-spanning receptors and heart function. Nature. 2002;415:206–212. - PubMed
-
- Pierce KL, Premont RT, Lefkowitz RJ. Seven-transmembrane receptors. Nat Rev Mol Cell Biol. 2002;3:639–650. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
