

Acute doxorubicin cardiotoxicity is associated with p53-induced inhibition of the mammalian target of rapamycin pathway
- PMID: 19103993
- PMCID: PMC2630181
- DOI: 10.1161/CIRCULATIONAHA.108.799700
Acute doxorubicin cardiotoxicity is associated with p53-induced inhibition of the mammalian target of rapamycin pathway
Abstract
Background: Doxorubicin is used to treat childhood and adult cancer. Doxorubicin treatment is associated with both acute and chronic cardiotoxicity. The cardiotoxic effects of doxorubicin are cumulative, which limits its chemotherapeutic dose. Free radical generation and p53-dependent apoptosis are thought to contribute to doxorubicin-induced cardiotoxicity.
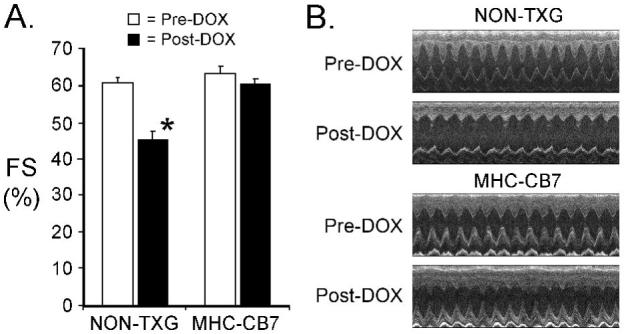
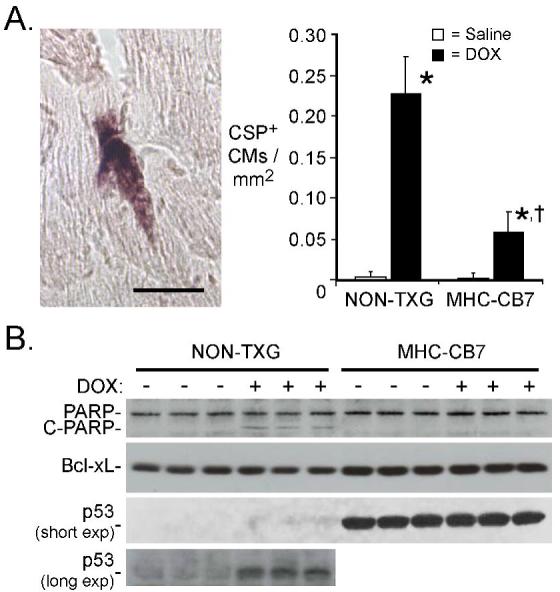
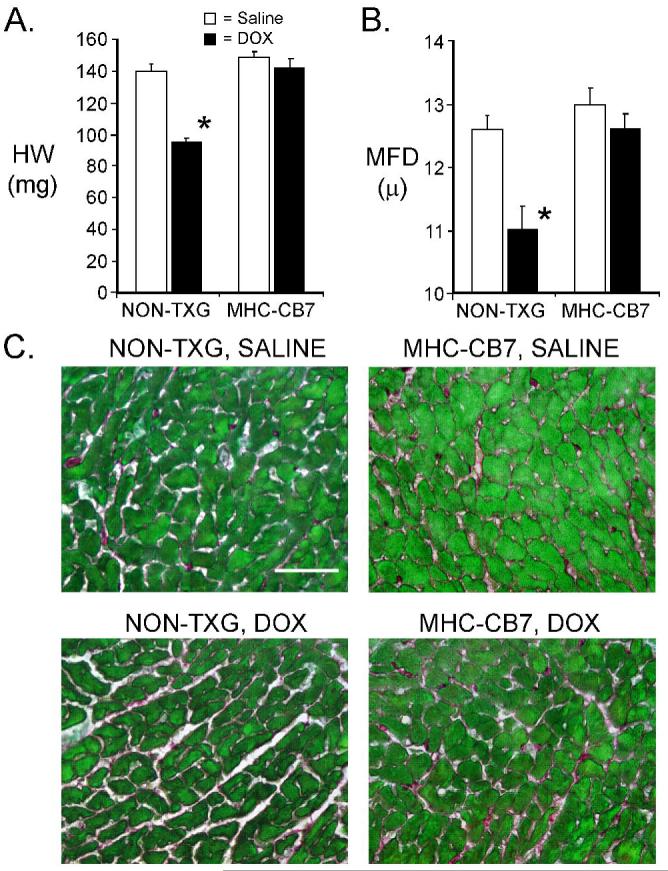
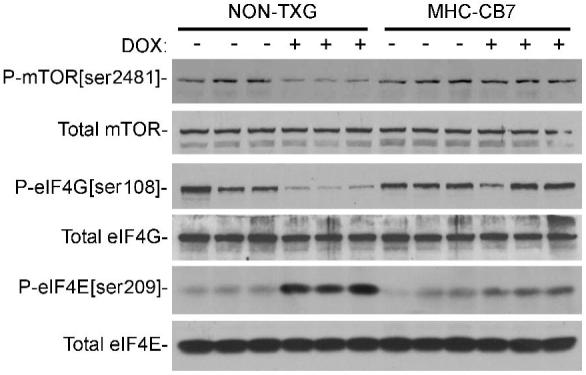
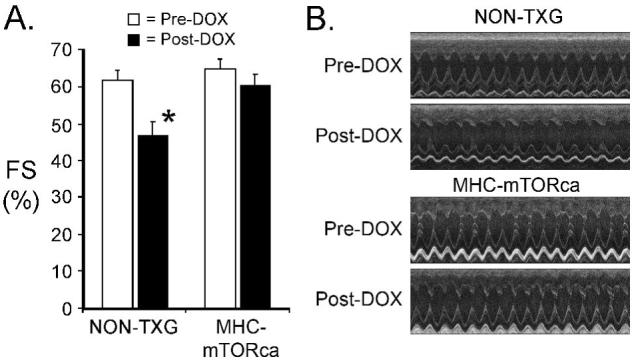
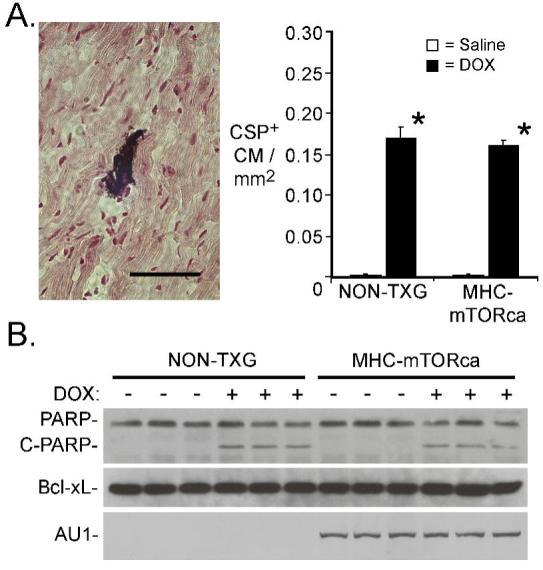
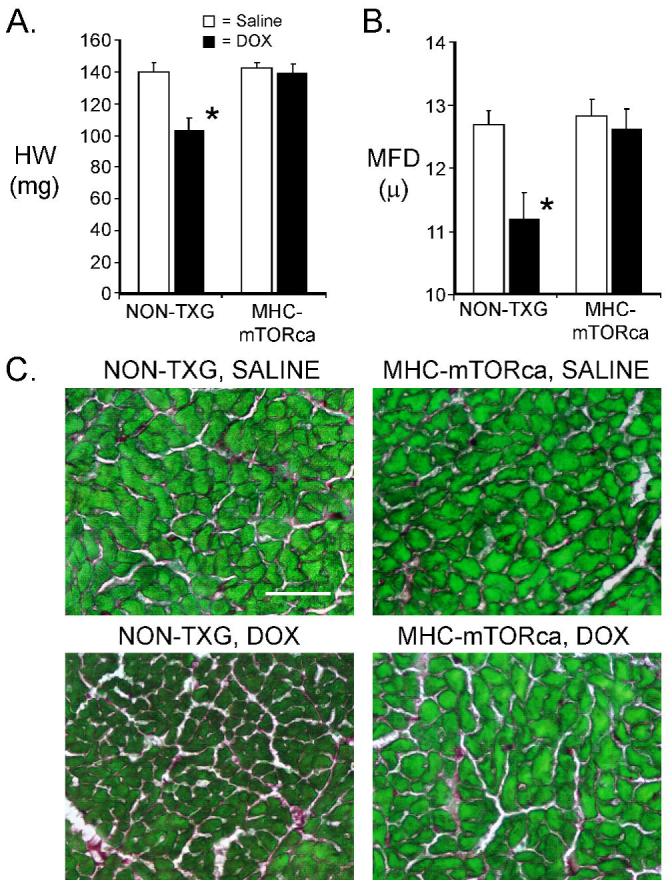
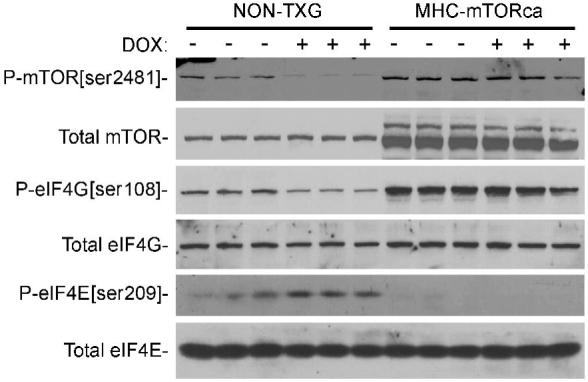
Methods and results: Adult transgenic (MHC-CB7) mice expressing cardiomyocyte-restricted dominant-interfering p53 and their nontransgenic littermates were treated with doxorubicin (20 mg/kg cumulative dose). Nontransgenic mice exhibited reduced left ventricular systolic function (predoxorubicin fractional shortening [FS] 61+/-2%, postdoxorubicin FS 45+/-2%, mean+/-SEM, P<0.008), reduced cardiac mass, and high levels of cardiomyocyte apoptosis 7 days after the initiation of doxorubicin treatment. In contrast, doxorubicin-treated MHC-CB7 mice exhibited normal left ventricular systolic function (predoxorubicin FS 63+/-2%, postdoxorubicin FS 60+/-2%, P>0.008), normal cardiac mass, and low levels of cardiomyocyte apoptosis. Western blot analyses indicated that mTOR (mammalian target of rapamycin) signaling was inhibited in doxorubicin-treated nontransgenic mice but not in doxorubicin-treated MHC-CB7 mice. Accordingly, transgenic mice with cardiomyocyte-restricted, constitutively active mTOR expression (MHC-mTORca) were studied. Left ventricular systolic function (predoxorubicin FS 64+/-2%, postdoxorubicin FS 60+/-3%, P>0.008) and cardiac mass were normal in doxorubicin-treated MHC-mTORca mice, despite levels of cardiomyocyte apoptosis similar to those seen in doxorubicin-treated nontransgenic mice.
Conclusions: These data suggest that doxorubicin treatment induces acute cardiac dysfunction and reduces cardiac mass via p53-dependent inhibition of mTOR signaling and that loss of myocardial mass, and not cardiomyocyte apoptosis, is the major contributor to acute doxorubicin cardiotoxicity.
Figures
References
-
- Bristow MR, Billingham ME, Mason JW, Daniels JR. Clinical spectrum of anthracycline antibiotic cardiotoxicity. Cancer Treat Rep. 1978;62(6):873–879. - PubMed
-
- Lefrak EA, Pitha J, Rosenheim S, Gottlieb JA. A clinicopathologic analysis of adriamycin cardiotoxicity. Cancer. 1973;32(2):302–314. - PubMed
-
- Lipshultz SE, Alvarez JA, Scully RE. Anthracycline associated cardiotoxicity in survivors of childhood cancer. Heart. 2008;94(4):525–533. - PubMed
-
- Singal PK, Iliskovic N. Doxorubicin-induced cardiomyopathy. N Engl J Med. 1998;339(13):900–905. - PubMed
-
- Zhou S, Starkov A, Froberg MK, Leino RL, Wallace KB. Cumulative and irreversible cardiac mitochondrial dysfunction induced by doxorubicin. Cancer Res. 2001;61(2):771–777. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
