

Primary prophylaxis in children with haemophilia
- PMID: 19105503
- PMCID: PMC2652217
- DOI: 10.2450/2008.0030-08
Primary prophylaxis in children with haemophilia
Abstract
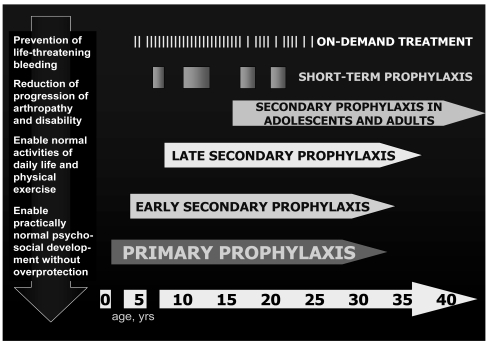
Starting from the clinical observations that moderate haemophiliacs experienced only few bleeding episodes and rarely developed significant joint deterioration (haemophilic arthropathy), and the pioneer experience in Sweden, prophylaxis (i.e. the regular and long-term administration of clotting factor concentrate in order to prevent bleeding) has been practiced for more than forty years in severe haemophilia and is currently recommended as the first choice of treatment by the World Health Organisation and World Federation of Hemophilia and by many national medical/scientific organizations. Observational studies clearly established the superiority of prophylaxis over on-demand treatment in reducing the risk of arthropathy, also showing that starting prophylaxis earlier in life and after very few joint bleeds was associated with better joint outcomes, and led to the current definitions of primary (started before the age of 2 yrs and after no more than one joint bleed) and secondary prophylaxis. More recently, evidences from randomized trials, which were previously lacking in this setting, were also provided. This review summarizes available data from which current clinical practice of primary (and early secondary) prophylaxis in children with severe haemophilia was drawn. Open issues concerning optimal regimens and barriers to the implementation of prophylaxis are also discussed.
Figures
Similar articles
-
Secondary prophylaxis in adolescent and adult haemophiliacs.Blood Transfus. 2008 Sep;6 Suppl 2(Suppl 2):s17-20. doi: 10.2450/2008.0032-08. Blood Transfus. 2008. PMID: 19105505 Free PMC article. Review.
-
Prophylaxis for severe haemophilia: clinical and economical issues.Haemophilia. 2003 Jul;9(4):376-81. doi: 10.1046/j.1365-2516.2003.00764.x. Haemophilia. 2003. PMID: 12828671
-
The overall effectiveness of prophylaxis in severe haemophilia.Haemophilia. 2003 May;9(3):272-8. doi: 10.1046/j.1365-2516.2003.00757.x. Haemophilia. 2003. PMID: 12694517
-
[Prevention of joint damage in hemophilic children with early prophylaxis].Orthopade. 1999 Apr;28(4):341-6. doi: 10.1007/PL00003616. Orthopade. 1999. PMID: 10335528 Clinical Trial. German.
-
The treatment of haemophilia, including prophylaxis, constant infusion and DDAVP.Baillieres Clin Haematol. 1996 Jun;9(2):259-71. doi: 10.1016/s0950-3536(96)80062-x. Baillieres Clin Haematol. 1996. PMID: 8800504 Review.
Cited by
-
A novel B-domain O-glycoPEGylated FVIII (N8-GP) demonstrates full efficacy and prolonged effect in hemophilic mice models.Blood. 2013 Mar 14;121(11):2108-16. doi: 10.1182/blood-2012-01-407494. Epub 2013 Jan 18. Blood. 2013. PMID: 23335368 Free PMC article.
-
Alloantibodies to therapeutic factor VIII in hemophilia A: the role of von Willebrand factor in regulating factor VIII immunogenicity.Haematologica. 2015 Feb;100(2):149-56. doi: 10.3324/haematol.2014.112821. Haematologica. 2015. PMID: 25638804 Free PMC article. Review.
-
Current therapeutic approaches in the management of hemophilia-a consensus view by the Romanian Society of Hematology.Ann Transl Med. 2021 Jul;9(13):1091. doi: 10.21037/atm-21-747. Ann Transl Med. 2021. PMID: 34423003 Free PMC article. Review.
-
Secondary prophylaxis in adolescent and adult haemophiliacs.Blood Transfus. 2008 Sep;6 Suppl 2(Suppl 2):s17-20. doi: 10.2450/2008.0032-08. Blood Transfus. 2008. PMID: 19105505 Free PMC article. Review.
-
Assessment of the impact of treatment on quality of life of patients with haemophilia A at different ages: insights from two clinical trials on turoctocog alfa.Haemophilia. 2014 Jul;20(4):527-34. doi: 10.1111/hae.12371. Epub 2014 Jan 29. Haemophilia. 2014. PMID: 24471912 Free PMC article. Clinical Trial.
References
-
- Nilsson IM, Berntorp E, Löfqvist T, Pettersson H. Twenty-five years experience of prophylactic treatment in severe haemophilia A and B. J Intern Med. 1992;232:25–32. - PubMed
-
- Ramgren O. Haemophilia in Sweden. III. Symptomatology, with special reference to differences between haemophilia A and B. Acta Med Scand. 1962;171:237–42. - PubMed
-
- Ahlberg A. Haemophilia in Sweden. VII. Incidence, treatment and prophylaxis of arthropathy and other musculo-skeletal manifestations of haemophilia A and B. Acta Orthop Scand Suppl. 1965;(Suppl 77):3–132. - PubMed
-
- Aledort L, Haschmeyer RH, Pettersson H. A longitudinal study of orthopaedic outcomes for severe factor-VIII-deficient haemophiliacs. The Orthopaedic Outcome Study Group. J Intern Med. 1994;236:391–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
