

Case mix, outcome and activity for patients with severe acute kidney injury during the first 24 hours after admission to an adult, general critical care unit: application of predictive models from a secondary analysis of the ICNARC Case Mix Programme database
- PMID: 19105800
- PMCID: PMC2607110
- DOI: 10.1186/cc7003
Case mix, outcome and activity for patients with severe acute kidney injury during the first 24 hours after admission to an adult, general critical care unit: application of predictive models from a secondary analysis of the ICNARC Case Mix Programme database
Abstract
Introduction: This study pools data from the UK Intensive Care National Audit and Research Center (ICNARC) Case Mix Programme (CMP) to evaluate the case mix, outcome and activity for 17,326 patients with severe acute kidney injury (AKI) occurring during the first 24 hours of admission to intensive care units (ICU).
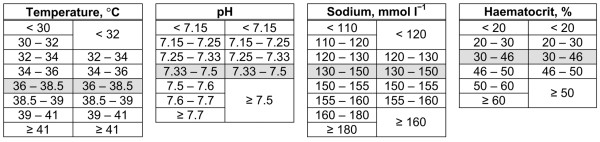
Methods: Severe AKI admissions (defined as serum creatinine >/=300 mumol/l and/or urea >/=40 mmol/l during the first 24 hours) were extracted from the ICNARC CMP database of 276,326 admissions to UK ICUs from 1995 to 2004. Subgroups of oliguric and nonoliguric AKI were identified by daily urine output. Data on surgical status, survival and length of stay were also collected. Severity of illness scores and mortality prediction models were compared (UK Acute Physiology and Chronic Health Evaluation [APACHE] II, Stuivenberg Hospital Acute Renal Failure [SHARF] T0, SHARF II0 and the Mehta model).
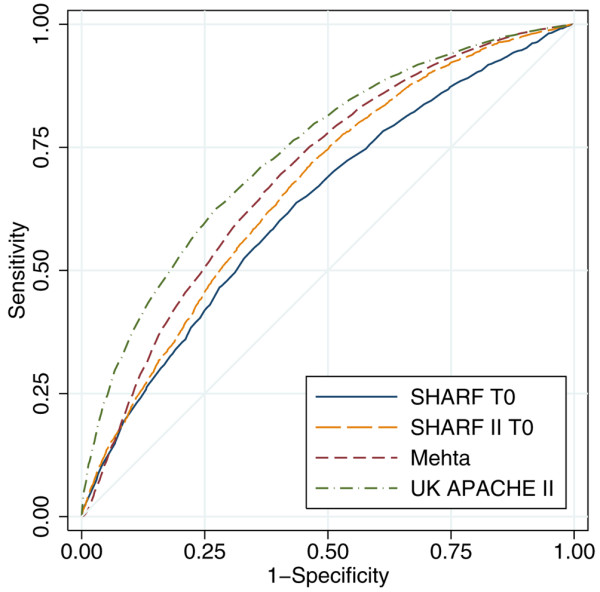
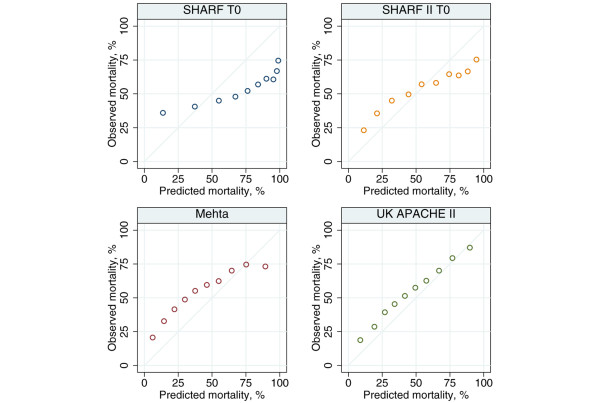
Results: Severe AKI occurred in 17,326 out of 276,731 admissions (6.3%). The source of admission was nonsurgical in 83.7%. Sepsis was present in 47.3% and AKI was nonoliguric in 63.9% of cases. Admission to ICU with severe AKI accounted for 9.3% of all ICU bed-days. Oliguric AKI was associated with longer length of stay for survivors and shorter length of stay for nonsurvivors compared with nonoliguric AKI. Oliguric AKI was associated with significantly greater ICU and hospital mortality (55.8% and 77.3%, respectively) compared with nonoliguric AKI (33.4% and 49.3%, respectively). Surgery during the 1 week before admission or during the first week in the CMP unit was associated with decreased odds of mortality. UK APACHE II and the Mehta scores under-predicted the number of deaths, whereas SHARF T0 and SHARF II0 over-predicted the number of deaths.
Conclusions: Severe AKI accounts for over 9% of all bed-days in adult, general ICUs, representing a considerable drain on resources. Although nonoliguric AKI continues to confer a survival benefit, overall survival from AKI in the ICU and survival to leave hospital remains poor. The use of APACHE II score measured during the first 24 hours of ICU stay performs well as compared with SHARF T0, SHARF II0 and the Mehta score, but it lacks perfect calibration.
Figures
Comment in
-
Acute kidney injury on admission to the intensive care unit: where to go from here?Crit Care. 2008;12(6):189. doi: 10.1186/cc7096. Epub 2008 Nov 7. Crit Care. 2008. PMID: 19090977 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
