

Cost-effectiveness of combination therapy for chronic obstructive pulmonary disease
- PMID: 19107245
- PMCID: PMC2682167
- DOI: 10.1155/2008/257618
Cost-effectiveness of combination therapy for chronic obstructive pulmonary disease
Abstract
Background: There is evidence that combination therapy (CT) in the form of long-acting beta(2)-agonists (LABAs) and inhaled corticosteroids can improve lung function for patients with chronic obstructive pulmonary disease (COPD).
Objective: To determine the cost-effectiveness of using CT in none, all or a selected group of COPD patients.
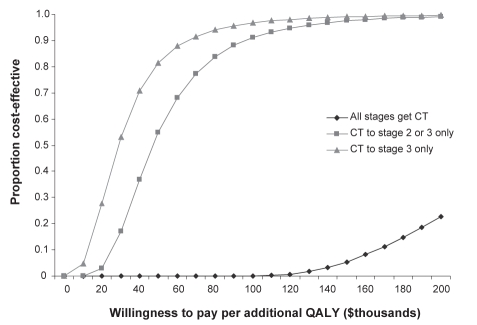
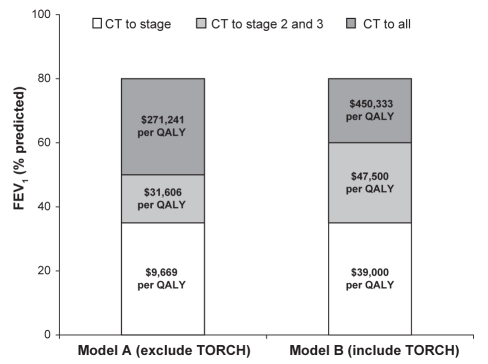
Methods: A Markov model was designed to compare four treatment strategies: no use of CT regardless of COPD severity (patients receive LABA only); use of CT in patients with stage 3 disease only (forced expiratory volume in 1 s [FEV(1)] less than 35% of predicted); use of CT in patients with stages 2 and 3 disease only (FEV(1) less than 50% of predicted); and use of CT in all patients regardless of severity of COPD. Estimates of mortality, exacerbation and disease progression rates, quality- adjusted life years (QALYs) and costs were derived from the literature. Three-year and lifetime time horizons were used. The analysis was conducted from a health systems perspective.
Results: CT was associated with a cost of $39,000 per QALY if given to patients with stage 3 disease, $47,500 per QALY if given to patients with stages 2 and 3 disease, and $450,333 per QALY if given to all COPD patients. Results were robust to various assumptions tested in a Monte Carlo simulation.
Conclusion: Providing CT for COPD patients in stage 2 or 3 disease is cost-effective. The message to family physicians and specialists is that as FEV(1) worsens and reaches 50% of predicted values, CT is recommended.
HISTORIQUE :: Selon certaines données probantes, la polythérapie sous forme de bêta2-agonistes à action prolongée (BAAP) et de corticoïdes par aérosol peut améliorer la fonction pulmonaire des patients atteints d’une maladie pulmonaire obstructive chronique (MPOC).
OBJECTIF :: Déterminer le rapport coût-efficacité de l’utilisation de la polythérapie chez aucun patient atteint de MPOC, tous les patients atteints de MPOC ou certains de ces patients.
MÉTHODOLOGIE :: Les auteurs ont conçu un modèle de Markov pour comparer quatre stratégies de traitement : ne pas recourir à la polythérapie, quelle que soit la gravité de la maladie (les patients ne reçoivent que des BAAP), recourir à la polythérapie seulement chez les patients atteints d’une MPOC de phase 3 (volume expiratoire maximal par seconde [VEMS] inférieur à 35 % de celui prévu), utilisation de la polythérapie seulement en présence d’une maladie de phase 2 ou 3 (VEMS inférieur à 50 % de celui prévu) et recourir à la polythérapie chez tous les patients quelle que soit la gravité de la MPOC. Les auteurs ont dérivé des publications les estimations des taux de mortalité, d’exacerbation et d’évolution du diagnostic, les années de vie pondérée par la qualité (AVPQ) et les coûts. Ils ont utilisé un horizon prévisionnel de trois ans et d’une vie entière. Ils ont effectué l’analyse selon la perspective du système de santé.
RÉSULTATS :: La polythérapie s’associe à un coût de 39 000 $ par AVPQ si elle est administrée aux patients atteints de la maladie de phase trois, de 47 500 $ par AVPQ si elle est administrée aux patients atteints de la maladie de phase 2 ou 3, et de 450 333 $ par AVPQ si elle est administrée à tous les patients atteints d’une MPOC. Les résultats résistaient à diverses hypothèses vérifiées dans une simulation de Monte Carlo.
CONCLUSION :: L’administration d’une polythérapie aux patients atteints d’une MPOC de phase 2 ou 3 est rentable. Le message à transmettre aux médecins de famille et aux spécialistes, c’est que lorsque le VEMS s’aggrave et atteint 50 %, la polythérapie est recommandée.
Figures
References
-
- Global Initiative for Chronic Obstructive Pulmonary Disease Global Initiative for Chronic Obstructive lung disease global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2006) 2006.
-
- Sullivan SD, Ramsey SD, Lee TA. The economic burden of COPD. Chest. 2000;117:5S–9S. - PubMed
-
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global burden of disease study. Lancet. 1997;349:1498–504. - PubMed
-
- Michaud CM, Murray CJ. Burden of disease-implications for future research. JAMA. 2001;285:535–9. - PubMed
-
- Shukla VK, Husereau DR, Boucher M, et al. Technology Report no 27. Ottawa: Canadian Coordinating Office for Health Technology Assessment; 2002. Long-acting β2-agonists for maintenance therapy of stable chronic obstructive pulmonary disease: A systematic review.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
