

The 'single big cryoballoon' technique for acute pulmonary vein isolation in patients with paroxysmal atrial fibrillation: a prospective observational single centre study
- PMID: 19109353
- PMCID: PMC2655313
- DOI: 10.1093/eurheartj/ehn570
The 'single big cryoballoon' technique for acute pulmonary vein isolation in patients with paroxysmal atrial fibrillation: a prospective observational single centre study
Abstract
Aims: Cryothermal energy (CTE) ablation via a balloon catheter (Arctic Front, Cryocath) represents a novel technology for pulmonary vein isolation (PVI). However, balloon-based PVI approaches are associated with phrenic nerve palsy (PNP). We investigated whether 'single big cryoballoon'-deployed CTE lesions can (i) achieve acute electrical PVI without left atrium (LA) imaging and (ii) avoid PNP in patients with paroxysmal atrial fibrillation (PAF).
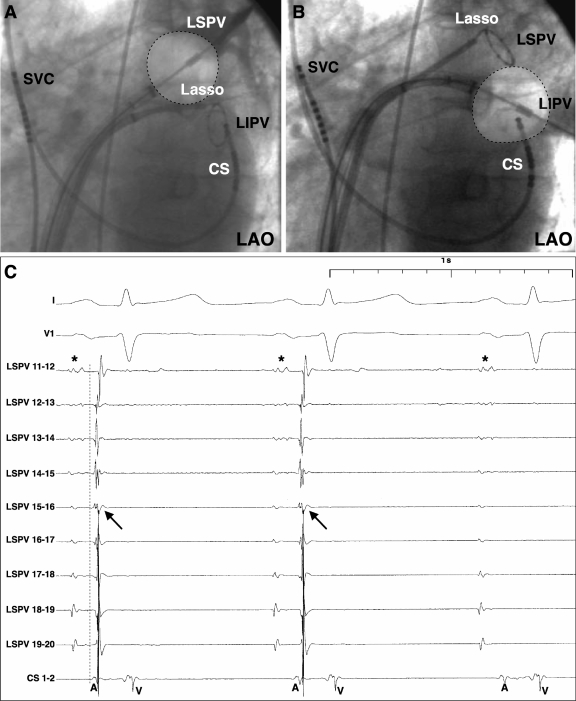
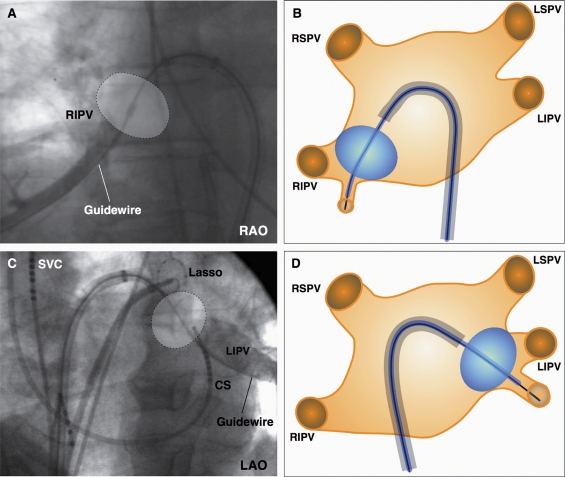
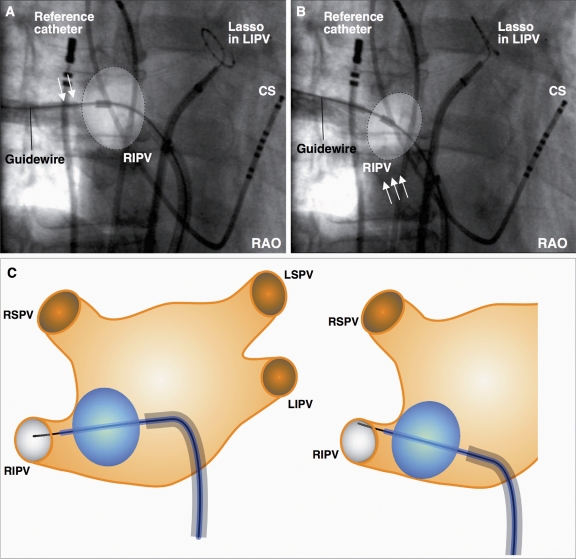
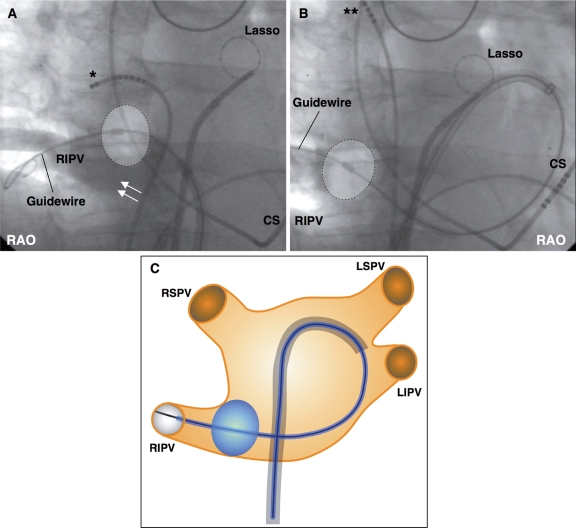
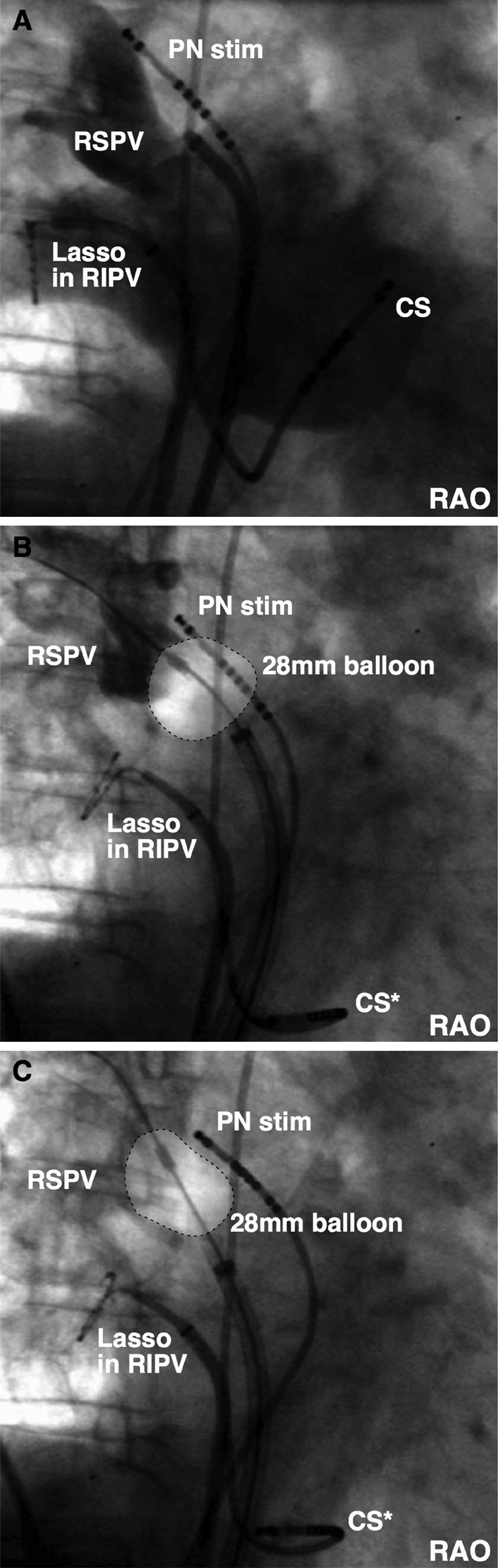
Methods and results: After double transseptal punctures, one Lasso catheter and a big 28 mm cryoballoon catheter using a steerable sheath were inserted into the LA. PV angiography and ostial Lasso recordings from all PVs were obtained. Selective PV angiography was used to evaluate balloon to LA-PV junction contact. CTE ablation lasted 300 s, and the PN was paced during freezing at right-sided PVs. Twenty-seven patients (19 males, mean age: 56 +/- 9 years, LA size: 42 +/- 5 mm) with PAF (mean duration: 6.6 +/- 5.7 years) were included. PVI was achieved in 97/99 PVs (98%). Median (Q(1); Q(3)) procedural, balloon, and fluoroscopy times were 220 min (190; 245), 130 min (90; 170), and 50 min (42; 69), respectively. Three transient PNP occurred after distal PV ablations. No PV stenosis occurred. Total median (Q(1); Q(3)) follow-up time was 271 days (147; 356), and 19 of 27 patients (70%) remained in sinus rhythm (3-month blanking period).
Conclusion: Using the single big cryoballoon technique, almost all PVs (98%) could be electrically isolated without LA imaging and may reduce the incidence of PNP as long as distal ablation inside the septal PVs is avoided.
Figures
Comment in
-
Cryoballoon ablation of paroxysmal atrial fibrillation: bigger is better and simpler is better.Eur Heart J. 2009 Mar;30(6):636-7. doi: 10.1093/eurheartj/ehp031. Epub 2009 Feb 17. Eur Heart J. 2009. PMID: 19223319 No abstract available.
References
-
- Haissaguerre M, Shah DC, Jais P, Hocini M, Yamane T, Deisenhofer I, Chauvin M, Garrigue S, Clementy J. Electrophysiological breakthroughs from the left atrium to the pulmonary veins. Circulation. 2000;14:2463–2465. - PubMed
-
- Oral H, Scharf C, Chugh A, Hall B, Cheung P, Good E, Veerareddy S, Pelosi F, Jr, Morady F. Catheter ablation for paroxysmal atrial fibrillation: segmental pulmonary vein ostial ablation versus left atrial ablation. Circulation. 2003;108:2355–2360. - PubMed
-
- Ouyang F, Bansch D, Ernst S, Schaumann A, Hachiya H, Chen M, Chun J, Falk P, Khanedani A, Antz M, Kuck KH. Complete isolation of left atrium surrounding the pulmonary veins: new insights from the double-Lasso technique in paroxysmal atrial fibrillation. Circulation. 2004;110:2090–2096. - PubMed
-
- Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. 2005;111:1100–1105. - PubMed
-
- Epstein MR, Knapp LD, Martindill M, Lulu JA, Triedmann JK, Calkins H, Huang SK, Walsh EP, Saul JP. Embolic complications associated with radiofrequency catheter ablation. Atakr Investigator Group. Am J Cardiol. 1996;77:655–658. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
