

Mechanisms of apnea
- PMID: 19110133
- PMCID: PMC3427748
- DOI: 10.1016/j.pcad.2008.02.003
Mechanisms of apnea
Abstract
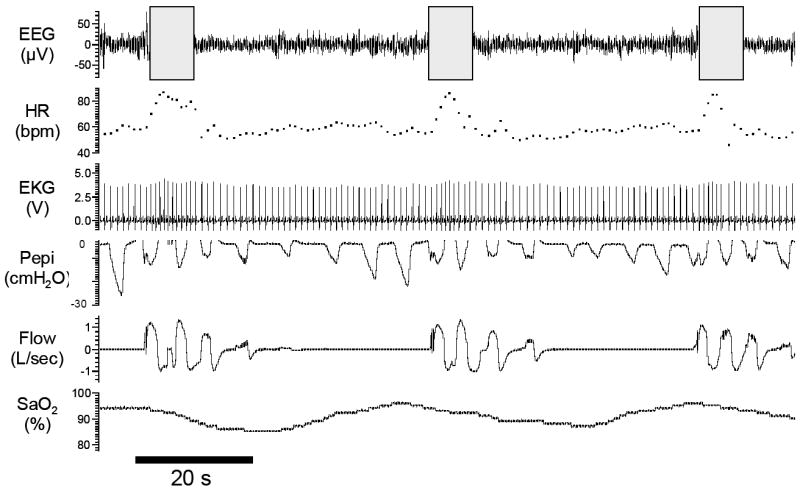
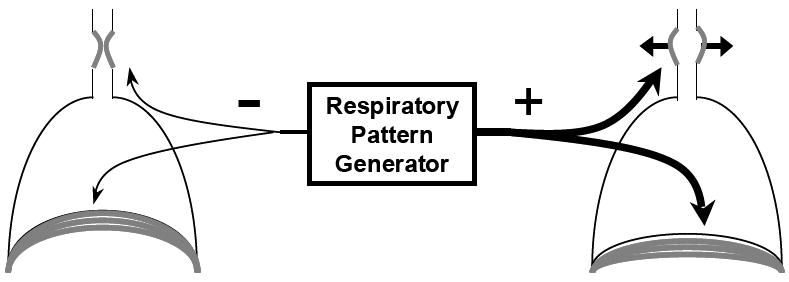
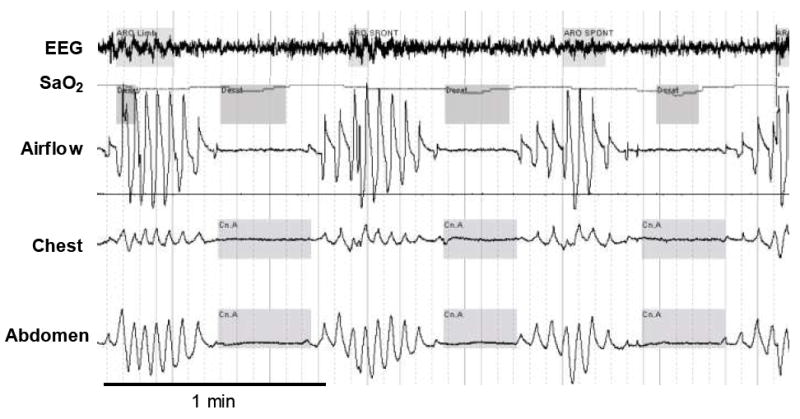
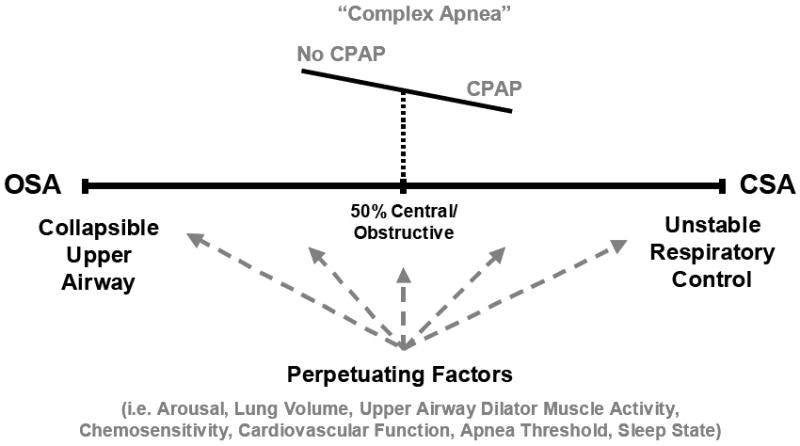
This paper focuses on the underlying mechanisms contributing to sleep-disordered breathing. Obstructive sleep apnea (OSA) is the most common sleep-related breathing disorder and is characterized by repetitive narrowing or collapse of the pharyngeal airway during sleep. Conversely, central sleep apnea (CSA), highly prevalent in congestive heart failure, is distinguished by a lack of drive to breathe during sleep, resulting in repetitive periods of insufficient ventilation. Both lead to compromised gas exchange, impaired sleep continuity, and catecholamine surges and are associated with major comorbidities including excessive daytime sleepiness and increased risk of cardiovascular disease. Although OSA and CSA exist on a spectrum of sleep-disordered breathing, the 2 entities may overlap in their underlying pathophysiologies. This brief review summarizes the etiology and current understanding of OSA and CSA pathophysiology and the role that the cardiovascular system may play in contributing to disease pathology and highlights the likely substantial overlap that exists between the various forms of sleep-disordered breathing.
Figures
References
-
- Punjabi NM, O’Hearn DJ, Neubauer DN, Nieto FJ, Schwartz AR, Smith PL, Bandeen-Roche K. Modeling hypersomnolence in sleep-disordered breathing. A novel approach using survival analysis. Am J Respir Crit Care Med. 1999;159:1703–1709. - PubMed
-
- Kim HC, Young T, Matthews CG, Weber SM, Woodward AR, Palta M. Sleep-disordered breathing and neuropsychological deficits. A population-based study. Am J Respir Crit Care Med. 1997;156:1813–1819. - PubMed
-
- Young T, Blustein J, Finn L, Palta M. Sleep-disordered breathing and motor vehicle accidents in a population- based sample of employed adults. Sleep. 1997;20:608–613. - PubMed
-
- Patil SP, Schneider H, Marx JJ, Gladmon E, Schwartz AR, Smith PL. Neuromechanical control of upper airway patency during sleep. J Appl Physiol. 2007;102:547–556. - PubMed
-
- Schwab RJ, Gupta KB, Gefter WB, Metzger LJ, Hoffman EA, Pack AI. Upper airway and soft tissue anatomy in normal subjects and patients with sleep-disordered breathing. Significance of the lateral pharyngeal walls. Am J Respir Crit Care Med. 1995;152:1673–1689. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
