

Mutations in DDR2 gene cause SMED with short limbs and abnormal calcifications
- PMID: 19110212
- PMCID: PMC2668047
- DOI: 10.1016/j.ajhg.2008.12.004
Mutations in DDR2 gene cause SMED with short limbs and abnormal calcifications
Abstract
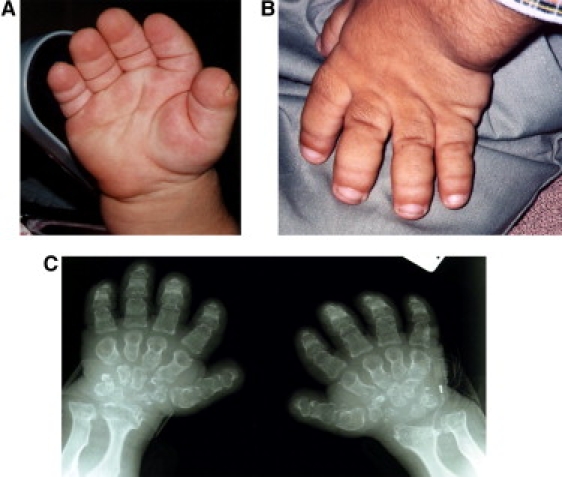
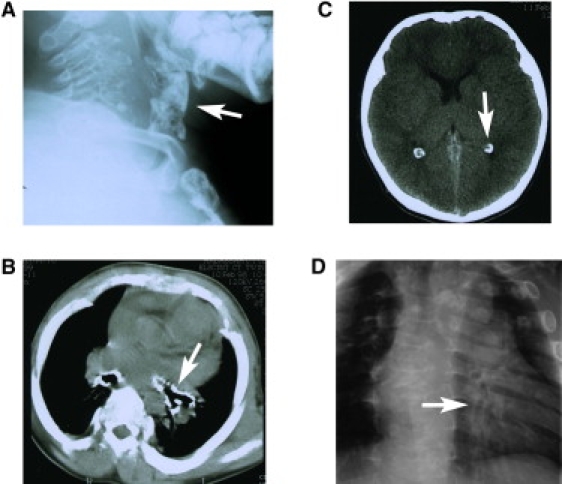
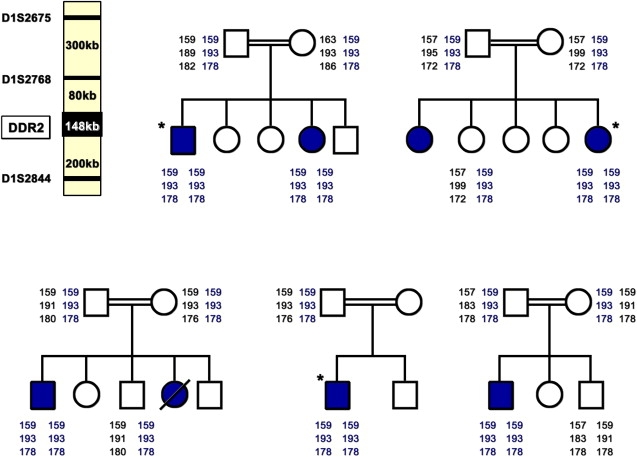
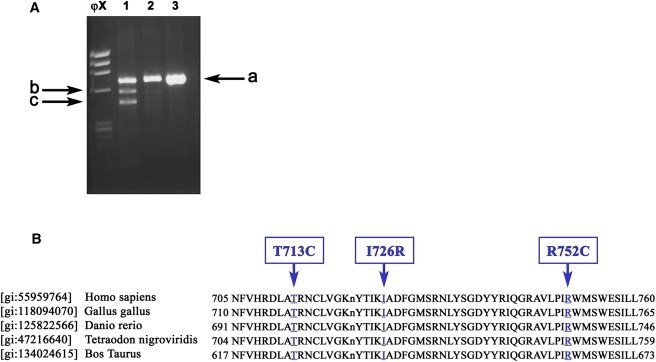
The spondylo-meta-epiphyseal dysplasia [SMED] short limb-hand type [SMED-SL] is a rare autosomal-recessive disease, first reported by Borochowitz et al. in 1993.(1) Since then, 14 affected patients have been reported.(2-5) We diagnosed 6 patients from 5 different consanguineous Arab Muslim families from the Jerusalem area with SMED-SL. Additionally, we studied two patients from Algerian and Pakistani ancestry and the parents of the first Jewish patients reported.(1) Using a homozygosity mapping strategy, we located a candidate region on chromosome 1q23 spanning 2.4 Mb. The position of the Discoidin Domain Receptor 2 (DDR2) gene within the candidate region and the similarity of the ddr2 knockout mouse to the SMED patients' phenotype prompted us to study this gene(6). We identified three missense mutations c.2254 C > T [R752C], c. 2177 T > G [I726R], c.2138C > T [T713I] and one splice site mutation [IVS17+1g > a] in the conserved sequence encoding the tyrosine kinase domain of the DDR2 gene. The results of this study will permit an accurate early prenatal diagnosis and carrier screening for families at risk.
Figures

References
-
- Borochowitz Z., Langer L.O., Jr., Gruber H.E., Lachman R., Katznelson M.B., Rimoin D.L. Spondylo-meta-epiphyseal dysplasia (SMED), short limb-hand type: A congenital familial skeletal dysplasia with distinctive features and histopathology. Am. J. Med. Genet. 1993;45:320–326. - PubMed
-
- Langer L.O., Jr., Wolfson B.J., Scott C.I., Jr., Reid C.S., Schidlow D.V., Millar E.A., Borns P.F., Lubicky J.P., Carpenter B.L. Further delineation of spondylo-meta-epiphyseal dysplasia, short limb-abnormal calcification type, with emphasis on diagnostic features. Am. J. Med. Genet. 1993;45:488–500. - PubMed
-
- Al-Gazali L.I., Bakalinova D., Sztriha L. Spondylo-meta-epiphyseal dysplasia, short limb, abnormal calcification type. Clin. Dysmorphol. 1996;5:197–206. - PubMed
-
- Fano V., Lejarraga H., Barreiro C. Spondylo-meta-epiphyseal dysplasia, short limbs, abnormal calcification type: A new case with severe neurological involvement. Pediatr. Radiol. 2001;31:19–22. - PubMed
-
- Tüysüz B., Gazioğlu N., Ungür S., Aji D.Y., Türkmen S. The time of onset of abnormal calcification in spondylometaepiphyseal dysplasia, short limb-abnormal calcification type. Pediatr. Radiol. 2009;39:84–89. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
