

Clinical patterns of obstructive sleep apnea and its comorbid conditions: a data mining approach
- PMID: 19110883
- PMCID: PMC2603531
Clinical patterns of obstructive sleep apnea and its comorbid conditions: a data mining approach
Abstract
Objectives: Obstructive sleep apnea often results in a wide range of comorbid conditions. Although some conditions have been clearly identified as comorbid, a full clinical pattern of associated diseases has not been systematically documented. This research aimed to reveal the full pattern of comorbid conditions associated with OSA by employing a data mining technique.
Methods: A large data repository (the New South Wales inpatient Data Collection) collected between 1999 and 2004 was mined, and all clinical diagnoses were coded with ICD-10-AM codes.
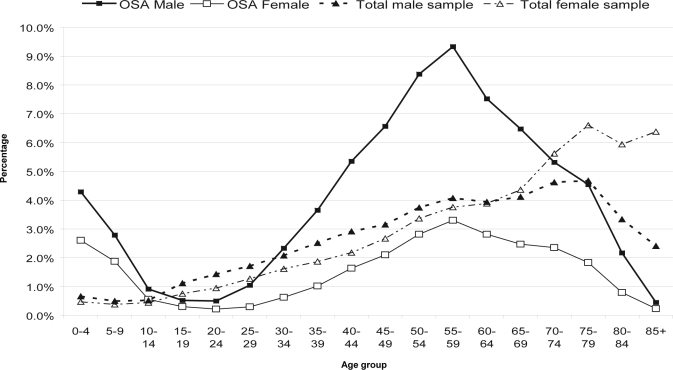
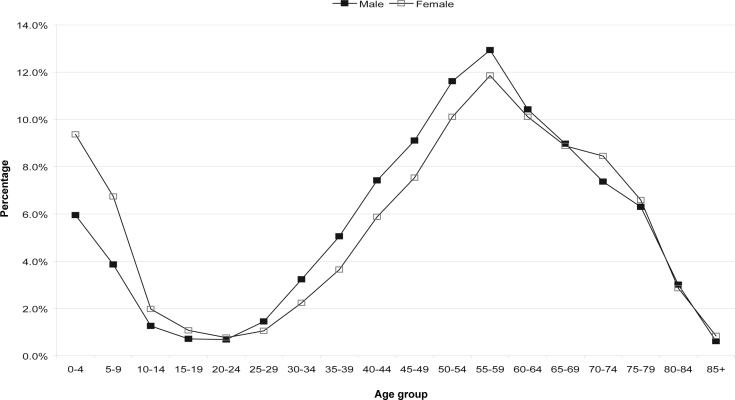
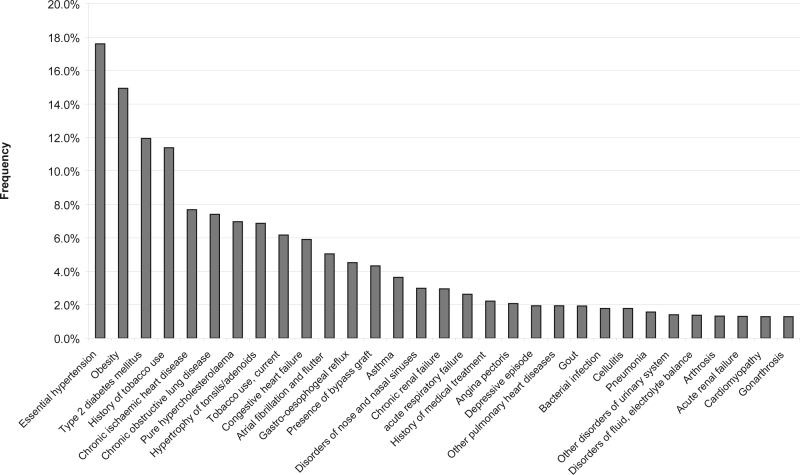
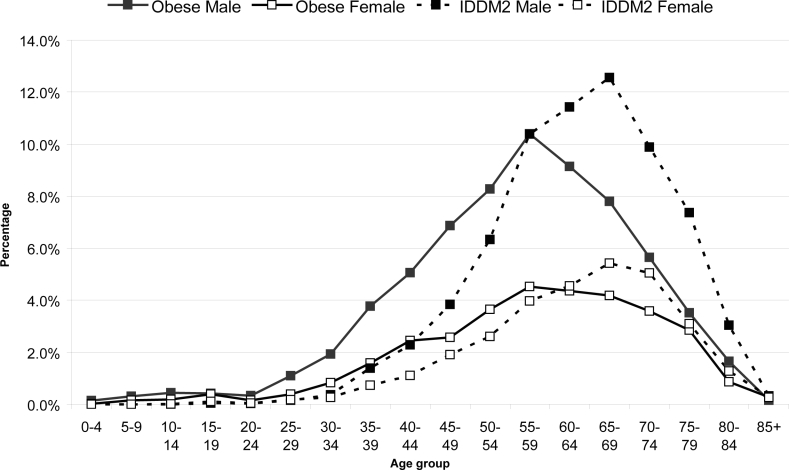
Results: A total of 60,197 cases (4% of total records) were identified as related to OSA (72.2% males, 27.8% females). OSA occurrence showed 2 peaks at 0-4 years and 55-59 years. A strikingly low occurrence was observed for the adolescent years. Conditions comorbid with OSA in adults by descending frequency were essential hypertension, obesity, hypercholesterolemia, type 2 diabetes, past or current tobacco use, and ischemic heart conditions. Obesity and OSA showed a similar time course of onset, with a latent period of 5 years for hypertension and type 2 diabetes and 15 years for chronic ischemic heart conditions. Comorbid conditions were predominantly of the cardiovascular, endocrine/metabolic and respiratory systems. The data also indicated OSA patients are high users of health services.
Conclusions: The data mining technique confirms the prevalence of the disease, describes the age distribution patterns and time courses of disease development from obesity and OSAto comorbid conditions, and implicates possible interrelationships among these conditions and high cost of treating OSA patients.
Figures



References
-
- Redline S, Kump K, Tishler PV, Browner I, Ferretter V. Gender differences in sleep disordered breathing in a community-based sample. Am J Respir Crit Care Med. 1994;149:722–26. - PubMed
-
- Krieger J, McNicholas W, Levy P, et al. Public health and medicolegal implications of sleep apnoea. Eur Respir J. 2002;20:1594–1609. - PubMed
-
- Young T, Skatrud J, Peppard PE. Risk factors for obstructive sleep apnea in adults. JAMA. 2004;291:2013–6. - PubMed
-
- Fayyad U, Piatetsky-Shapiro G, Smyth P. From data mining to knowledge discovery: an overview. In: Fayyad U, Piatetsky-Shapiro G, Smyth P, Uthurusamy R, editors. Advances in knowledge discovery and data mining. Menlo Park: Am Assoc Artificial Intelligence; 1996. pp. 37–54.
-
- Brossette SE, Sprague AP, Jones WT, et al. A data mining system for infection control surveillance. Methods Inf Med. 2000;39:303–10. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous