

Therapeutic hypothermia preserves antioxidant defenses after severe traumatic brain injury in infants and children
- PMID: 19114918
- PMCID: PMC2664386
- DOI: 10.1097/CCM.0b013e318194abf2
Therapeutic hypothermia preserves antioxidant defenses after severe traumatic brain injury in infants and children
Erratum in
- Crit Care Med. 2009 Apr;37(4):1536
Abstract
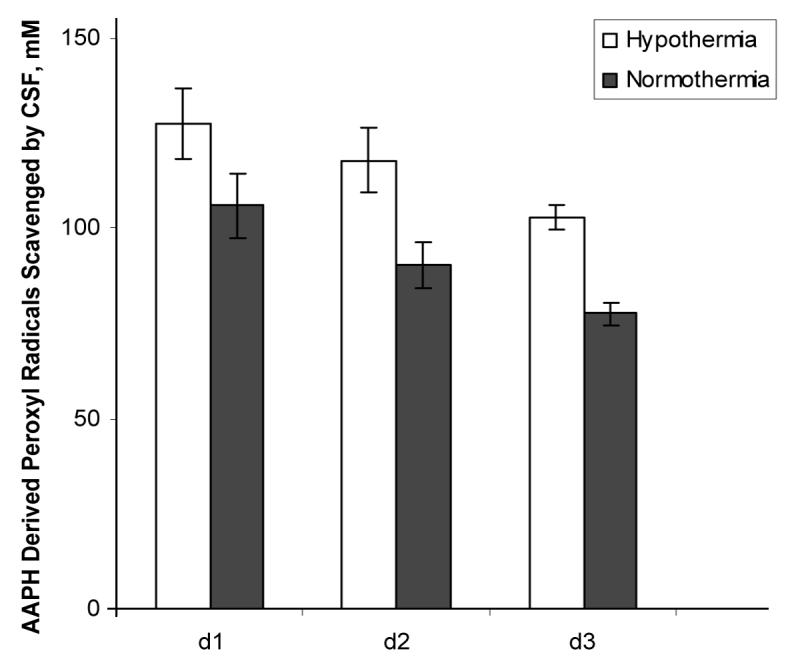
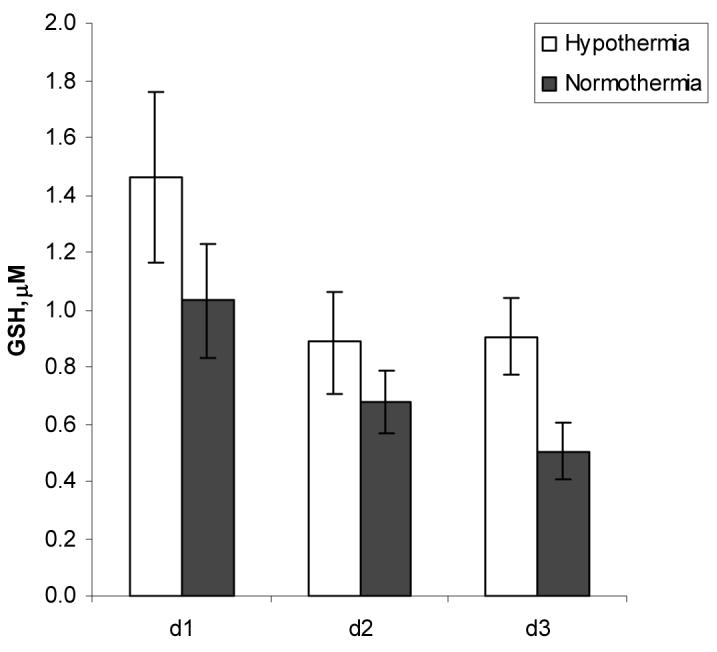
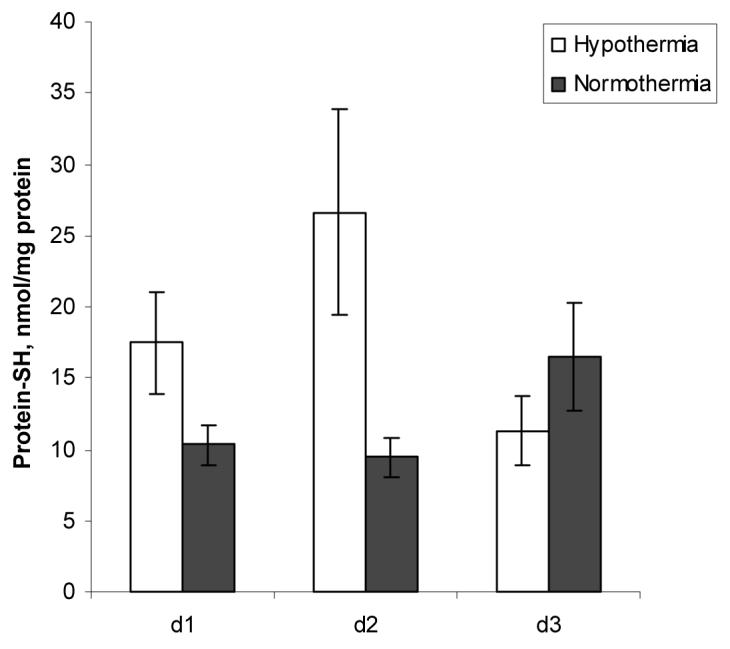
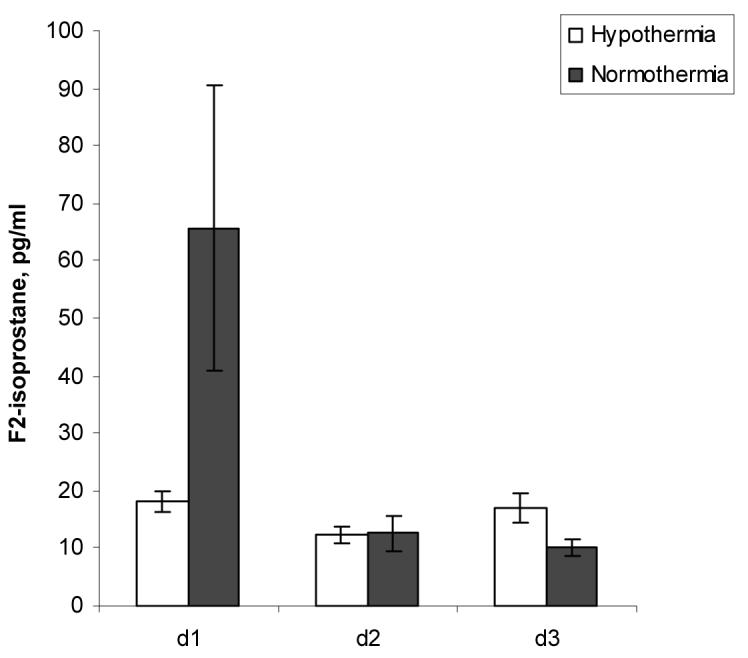
Objective: Oxidative stress contributes to secondary damage after traumatic brain injury (TBI). Hypothermia decreases endogenous antioxidant consumption and lipid peroxidation after experimental cerebral injury. Our objective was to determine the effect of therapeutic hypothermia on oxidative damage after severe TBI in infants and children randomized to moderate hypothermia vs. normothermia.
Design: Prospective randomized controlled study.
Setting: Pediatric intensive care unit of Pittsburgh Children's Hospital.
Patients: The study included 28 patients.
Measurements and main results: We compared the effects of hypothermia (32 degrees C-33 degrees C) vs. normothermia in patients treated in a single center involved in a multicentered randomized controlled trial of hypothermia in severe pediatric TBI (Glasgow Coma Scale score <or=8). The patients randomized to hypothermia (n = 13) were cooled to target temperature within approximately 6 to 24 hours for 48 hours and then rewarmed. Antioxidant status was assessed by measurements of total antioxidant reserve and glutathione. Protein oxidation and lipid peroxidation were assessed by measurements of protein thiols and F2-isoprostane, respectively, in ventricular cerebrospinal fluid (CSF) samples (n = 76) obtained on day 1-3 after injury. The association between Glasgow Coma Scale score, age, gender, treatment, temperature, time after injury, and CSF antioxidant reserve, glutathione, protein-thiol, F2-isoprostane levels were assessed by bivariate and multiple regression models. Demographic and clinical characteristics were similar between the two treatment groups. Mechanism of injury included both accidental injury and nonaccidental injury. Multiple regression models revealed preservation of CSF antioxidant reserve by hypothermia (p = 0.001). Similarly, a multiple regression model showed that glutathione levels were inversely associated with patient temperature at the time of sampling (p = 0.002). F2-isoprostane levels peaked on day 1 after injury and were progressively decreased thereafter. Although F2-isoprostane levels were approximately three-fold lower in patients randomized to hypothermia vs. normothermia, this difference was not statistically significant.
Conclusion: To our knowledge, this is the first study demonstrating that hypothermia attenuates oxidative stress after severe TBI in infants and children. Our data also support the concept that CSF represents a valuable tool for monitoring treatment effects on oxidative stress after TBI.
Figures
Comment in
-
Brain oxidative stress after traumatic brain injury ... cool it?Crit Care Med. 2009 Feb;37(2):787-8. doi: 10.1097/CCM.0b013e318194be10. Crit Care Med. 2009. PMID: 19325391 No abstract available.
References
-
- Adelson PD, Bratton SL, Carney NA, Chesnut RM, du Coudray HE, Goldstein B, Kochanek PM, Miller HC, Partington MD, Selden NR, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Chapter 8. Cerebral perfusion pressure. Pediatr Crit Care Med. 2003;4:S31–33. - PubMed
-
- Selden PD, Bratton SL, Carney NA, Chesnut RM, du Coudray HE, Goldstein B, Kochanek PM, Miller HC, Partington MD, Selden NR, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Chapter 14. The role of temperature control following severe pediatric traumatic brain injury. Pediatr Crit Care Med. 2003;4:S53–55. - PubMed
-
- Adelson PD, Ragheb J, Kanev P, Brockmeyer D, Beers SR, Brown SD, Cassidy LD, Chang Y, Levin H.Phase II clinical trial of moderate hypothermia after severe traumatic brain injury in children Neurosurgery 200556740–754.; discussion 740-754. - PubMed
-
- Biswas AK, Bruce DA, Sklar FH, Bokovoy JL, Sommerauer JF. Treatment of acute traumatic brain injury in children with moderate hypothermia improves intracranial hypertension. Crit Care Med. 2002;30:2742–2751. - PubMed
-
- Behringer W, Safar P, Kentner R, Wu X, Kagan VE, Radovsky A, Clark RS, Kochanek PM, Subramanian M, Tyurin VA, et al. Antioxidant Tempol enhances hypothermic cerebral preservation during prolonged cardiac arrest in dogs. J Cereb Blood Flow Metab. 2002;22:105–117. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- NS061817/NS/NINDS NIH HHS/United States
- HD057587/HD/NICHD NIH HHS/United States
- P50 NS030318/NS/NINDS NIH HHS/United States
- R01 NS061817/NS/NINDS NIH HHS/United States
- T32-HD40686/HD/NICHD NIH HHS/United States
- U01 NS052478/NS/NINDS NIH HHS/United States
- T32 HD040686/HD/NICHD NIH HHS/United States
- R01 NS038087/NS/NINDS NIH HHS/United States
- NS34884/NS/NINDS NIH HHS/United States
- NS052478/NS/NINDS NIH HHS/United States
- NS30318/NS/NINDS NIH HHS/United States
- P01 NS030318/NS/NINDS NIH HHS/United States
- NS38087/NS/NINDS NIH HHS/United States
- R21 HD057587/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
