

Use of integrated malaria management reduces malaria in Kenya
- PMID: 19115000
- PMCID: PMC2603594
- DOI: 10.1371/journal.pone.0004050
Use of integrated malaria management reduces malaria in Kenya
Erratum in
- PLoS One.2009; 4(2): 10.1371/annotation/e14952c5-b2db-4ff7-976d-6c794d275703
Abstract
Background: During an entomological survey in preparation for malaria control interventions in Mwea division, the number of malaria cases at the Kimbimbi sub-district hospital was in a steady decline. The underlying factors for this reduction were unknown and needed to be identified before any malaria intervention tools were deployed in the area. We therefore set out to investigate the potential factors that could have contributed to the decline of malaria cases in the hospital by analyzing the malaria control knowledge, attitudes and practices (KAP) that the residents in Mwea applied in an integrated fashion, also known as integrated malaria management (IMM).
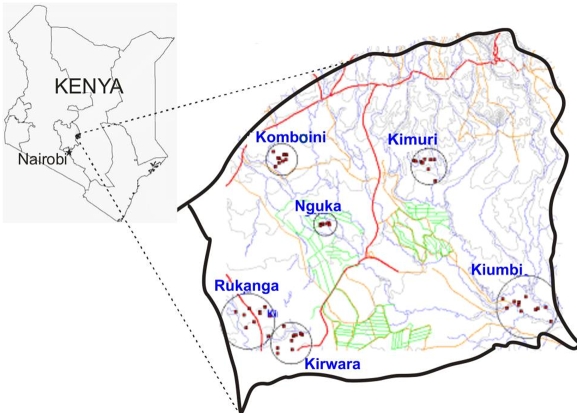
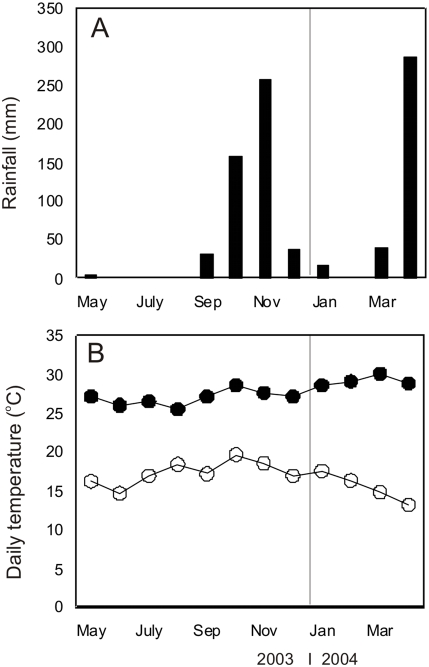
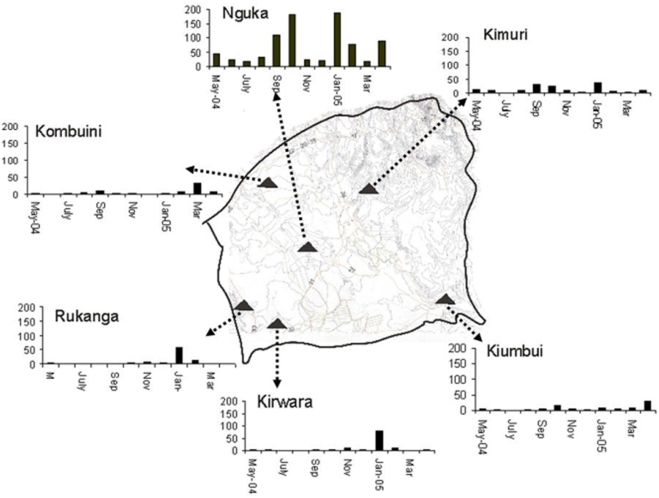
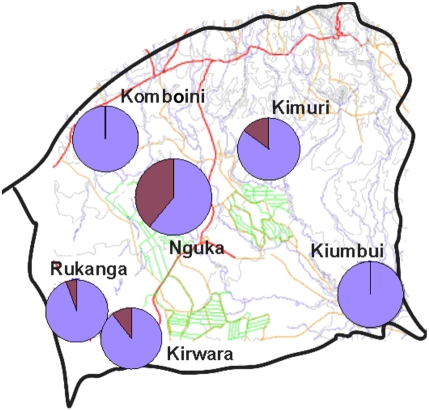
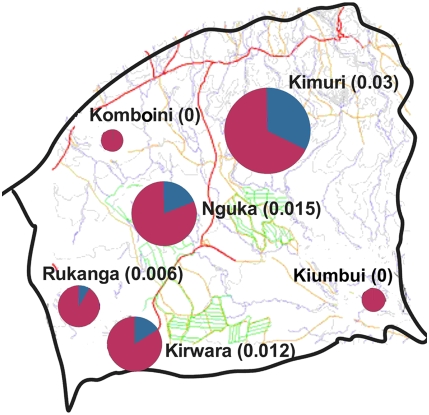
Methods: Integrated Malaria Management was assessed among community members of Mwea division, central Kenya using KAP survey. The KAP study evaluated community members' malaria disease management practices at the home and hospitals, personal protection measures used at the household level and malaria transmission prevention methods relating to vector control. Concurrently, we also passively examined the prevalence of malaria parasite infection via outpatient admission records at the major referral hospital in the area. In addition we studied the mosquito vector population dynamics, the malaria sporozoite infection status and entomological inoculation rates (EIR) over an 8 month period in 6 villages to determine the risk of malaria transmission in the entire division.
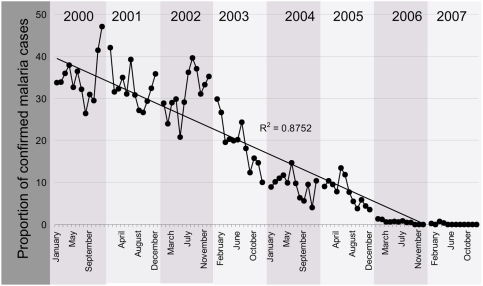
Results: A total of 389 households in Mwea division were interviewed in the KAP study while 90 houses were surveyed in the entomological study. Ninety eight percent of the households knew about malaria disease while approximately 70% of households knew its symptoms and methods to manage it. Ninety seven percent of the interviewed households went to a health center for malaria diagnosis and treatment. Similarly a higher proportion (81%) used anti-malarial medicines bought from local pharmacies. Almost 90% of households reported owning and using an insecticide treated bed net and 81% reported buying the nets within the last 5 years. The community also used mosquito reduction measures including, in order of preference, environmental management (35%), mosquito repellent and smoke (31%) insecticide canister sprays (11%), and window and door screens (6%). These methods used by the community comprise an integrated malaria management (IMM) package. Over the last 4 years prior to this study, the malaria cases in the community hospital reduced from about 40% in 2000 to less than 10% by 2004 and by the year 2007 malaria cases decreased to zero. In addition, a one time cross-sectional malaria parasite survey detected no Plasmodium infection in 300 primary school children in the area. Mosquito vector populations were variable in the six villages but were generally lower in villages that did not engage in irrigation activities. The malaria risk as estimated by EIR remained low and varied by village and proximity to irrigation areas. The average EIR in the area was estimated at 0.011 infectious bites per person per day.
Conclusions: The usage of a combination of malaria control tools in an integrated fashion by residents of Mwea division might have influenced the decreased malaria cases in the district hospital and in the school children. A vigorous campaign emphasizing IMM should be adopted and expanded in Mwea division and in other areas with different eco-epidemiological patterns of malaria transmission. With sustained implementation and support from community members integrated malaria management can reduce malaria significantly in affected communities in Africa.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
