

Subacute and chronic, non-specific back and neck pain: cognitive-behavioural rehabilitation versus primary care. A randomized controlled trial
- PMID: 19116007
- PMCID: PMC2649916
- DOI: 10.1186/1471-2474-9-172
Subacute and chronic, non-specific back and neck pain: cognitive-behavioural rehabilitation versus primary care. A randomized controlled trial
Abstract
Background: In the industrial world, non-specific back and neck pain (BNP) is the largest diagnostic group underlying sick-listing. For patients with subacute and chronic (= full-time sick-listed for 43 - 84 and 85 - 730 days, respectively) BNP, cognitive-behavioural rehabilitation was compared with primary care. The specific aim was to answer the question: within an 18-month follow-up, will the outcomes differ in respect of sick-listing and number of health-care visits?
Methods: After stratification by age (< or = 44/> or = 45 years) and subacute/chronic BNP, 125 Swedish primary-care patients were randomly allocated to cognitive-behavioural rehabilitation (rehabilitation group) or continued primary care (primary-care group). Outcome measures were Return-to-work share (percentage) and Return-to-work chance (hazard ratios) over 18 months, Net days (crude sick-listing days x degree), and the number of Visits (to physicians, physiotherapists etc.) over 18 months and the three component six-month periods. Descriptive statistics, Cox regression and mixed-linear models were used.
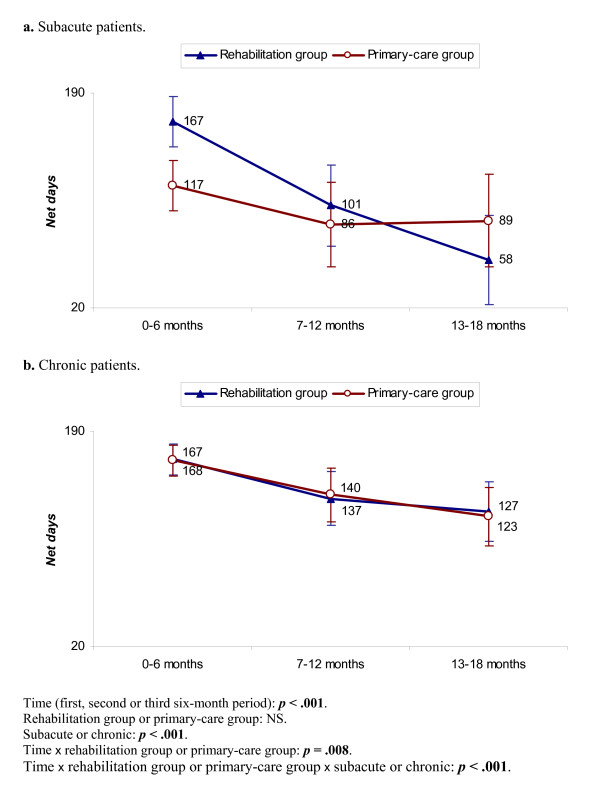
Results: All patients: Return-to-work share and Return-to-work chance were equivalent between the groups. Net days and Visits were equivalent over 18 months but decreased significantly more rapidly for the rehabilitation group over the six-month periods (p < .05). Subacute patients: Return-to-work share was equivalent. Return-to-work chance was significantly greater for the rehabilitation group (hazard ratio 3.5 [95%CI1.001 - 12.2]). Net days were equivalent over 18 months but decreased significantly more rapidly for the rehabilitation group over the six-month periods and there were 31 days fewer in the third period. Visits showed similar though non-significant differences and there were half as many in the third period. Chronic patients: Return-to-work share, Return-to-work chance and Net days were equivalent. Visits were equivalent over 18 months but tended to decrease more rapidly for the rehabilitation group and there were half as many in the third period (non-significant).
Conclusion: The results were equivalent over 18 months. However, there were indications that cognitive-behavioural rehabilitation in the longer run might be superior to primary care. For subacute BNP, it might be superior in terms of sick-listing and health-care visits; for chronic BNP, in terms of health-care visits only. More conclusive results concerning this possible long-term effect might require a longer follow-up.
Trial registration: ClinicalTrials.gov NCT00488735.
Figures




References
-
- Hansson T, Jensen I. Sickness absence due to back and neck disorders. In: Alexanderson K, Norlund A, editor. Sickness absence – causes, consequences, and physicians' sickness-certification practice Scand J Public Health. Vol. 32. 2004. pp. 109–151. - PubMed
-
- Nachemson A. Introduction. In: Nachemson A, Jonson E, editor. Neck and back pain The scientific evidence of causes, diagnosis, and treatment. Philadelphia: Lippincott, Williams & Williams; 2000. pp. 1–12.
-
- Norlund A, Waddell G. Cost of back pain in some OECD Countries. In: Nachemson A, Jonson E, editor. Neck and back pain The scientific evidence of causes, diagnosis, and treatment. Philadelphia: Lippincott, Williams & Williams; 2000. pp. 421–425.
-
- Waddell G, Watson PJ. Rehabilitation. In: Waddell G, editor. Back Pain Revolution. 2. Edinburgh: Churchill Livingstone; 2004. pp. 371–399.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
