

Primary lymphoma of the head and neck: two case reports and review of the literature
- PMID: 19116013
- PMCID: PMC2639388
- DOI: 10.1186/1757-1626-1-426
Primary lymphoma of the head and neck: two case reports and review of the literature
Abstract
Background: The head and neck is the second most common region for the extra-nodal lymphomas after that of gastrointestinal tract. Approximately 2.5% of malignant lymphoma arises in the oral and para-oral region. In this paper we report two cases of early stage head and neck lymphoma which were managed successfully with chemotherapy and a review of the related literature.
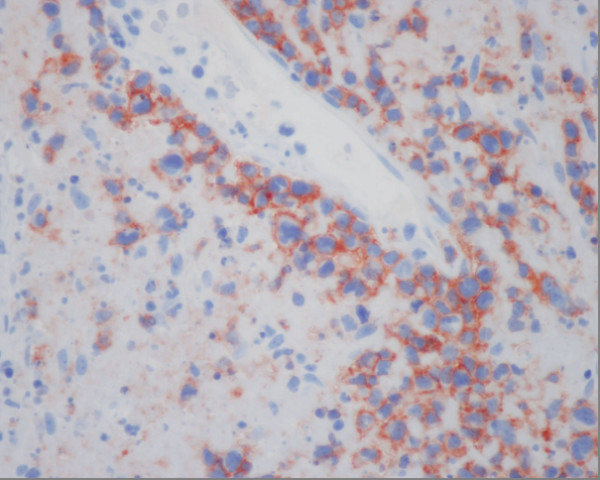
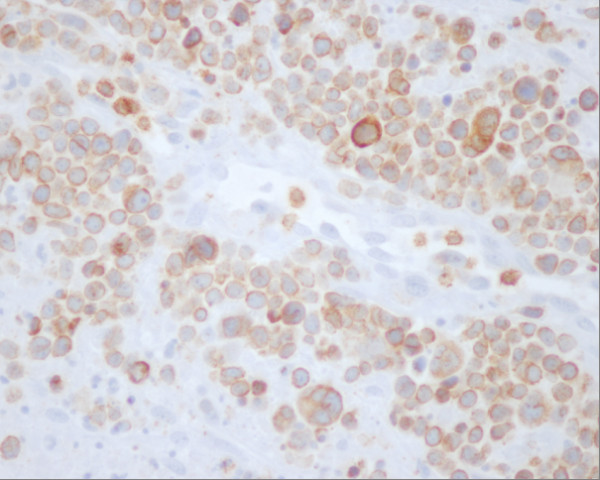
Cases presentation: The first case concerns a 48 years male patient having a diffuse large B-Cell lymphoma of the oropharynx at early bulky stage. This patient was managed successfully with 7 of Rituximab 375 mg/m2, Cyclophosphamide 750 mg/m2 d1, Doxorubicine 50 mg/m2 d1, Vincristine 1.4 mg/m2 d1, and prednisone 50 mg/m2 d1-5 (RCHOP) regimen. The second case concerns a 50 years female patient having the nasal natural killer (NK)/T-cell lymphoma of the left nasal pit at early stage. This case was managed successfully with 6 of Cyclophosphamide 750 mg/m2 d1, Doxorubicine 50 mg/m2 d1, Vincristine 1.4 mg/m2 d1, and prednisone 50 mg/m2 d1-5 (CHOP) regimen.
Conclusion: These two cases highlight the important role of CHOP based chemotherapy for achieving successful treatment cure for patients having an early stage head and neck lymphoma.
Figures





Similar articles
-
Primary lymphoma of the prostate treated with rituximab-based chemotherapy: a case report and review of the literature.Cases J. 2009 Aug 11;2:8875. doi: 10.1186/1757-1626-0002-0000008875. Cases J. 2009. PMID: 20184702 Free PMC article.
-
Superiority of second over first generation chemotherapy in a randomized trial for stage III-IV intermediate and high-grade non-Hodgkin's lymphoma (NHL): the 1980-1985 EORTC trial. The EORTC Lymphoma Group.Ann Oncol. 1991 Jun;2(6):431-5. doi: 10.1093/oxfordjournals.annonc.a057979. Ann Oncol. 1991. PMID: 1722697 Clinical Trial.
-
Role of chemotherapy in the management of primary rectal lymphoma: a case report and review of the literature.Cases J. 2009 Dec 22;2:9373. doi: 10.1186/1757-1626-2-9373. Cases J. 2009. PMID: 20062547 Free PMC article.
-
Cardiovascular adverse events in patients with non-Hodgkin lymphoma treated with first-line cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) or CHOP with rituximab (R-CHOP): a systematic review and meta-analysis.Lancet Haematol. 2020 Apr;7(4):e295-e308. doi: 10.1016/S2352-3026(20)30031-4. Epub 2020 Mar 2. Lancet Haematol. 2020. PMID: 32135128
-
The therapeutic use of rituximab in non-Hodgkin's lymphoma.Eur J Haematol Suppl. 2007 Jan;(67):5-14. doi: 10.1111/j.1600-0609.2006.00789.x. Eur J Haematol Suppl. 2007. PMID: 17206982 Review.
Cited by
-
Head and Neck Lymphoma in an Iranian Population.Iran J Otorhinolaryngol. 2017 Sep;29(94):262-267. Iran J Otorhinolaryngol. 2017. PMID: 31328112 Free PMC article.
-
Primary non-Hodgkin follicular lymphoma of the prostate: A case report.Turk J Urol. 2014 Mar;40(1):57-8. doi: 10.5152/tud.2014.68466. Turk J Urol. 2014. PMID: 26328148 Free PMC article.
-
Head and Neck Lymphoma in an Iranian Population.Iran J Otorhinolaryngol. 2017 Sep;29(94):261-267. Iran J Otorhinolaryngol. 2017. PMID: 29034220 Free PMC article.
-
Primary Nasopharyngeal non-Hodgkin lymphomas: a retrospective review of 26 Moroccan patients.BMC Ear Nose Throat Disord. 2009 Nov 17;9:11. doi: 10.1186/1472-6815-9-11. BMC Ear Nose Throat Disord. 2009. PMID: 19919708 Free PMC article.
-
Epiglottic diffuse B-cell malignant lymphoma: A case report.Mol Clin Oncol. 2016 Jan;4(1):58-60. doi: 10.3892/mco.2015.675. Epub 2015 Nov 9. Mol Clin Oncol. 2016. PMID: 26870358 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
