

Using a count of neonatal morbidities to predict poor outcome in extremely low birth weight infants: added role of neonatal infection
- PMID: 19117897
- PMCID: PMC2829863
- DOI: 10.1542/peds.2008-0377
Using a count of neonatal morbidities to predict poor outcome in extremely low birth weight infants: added role of neonatal infection
Abstract
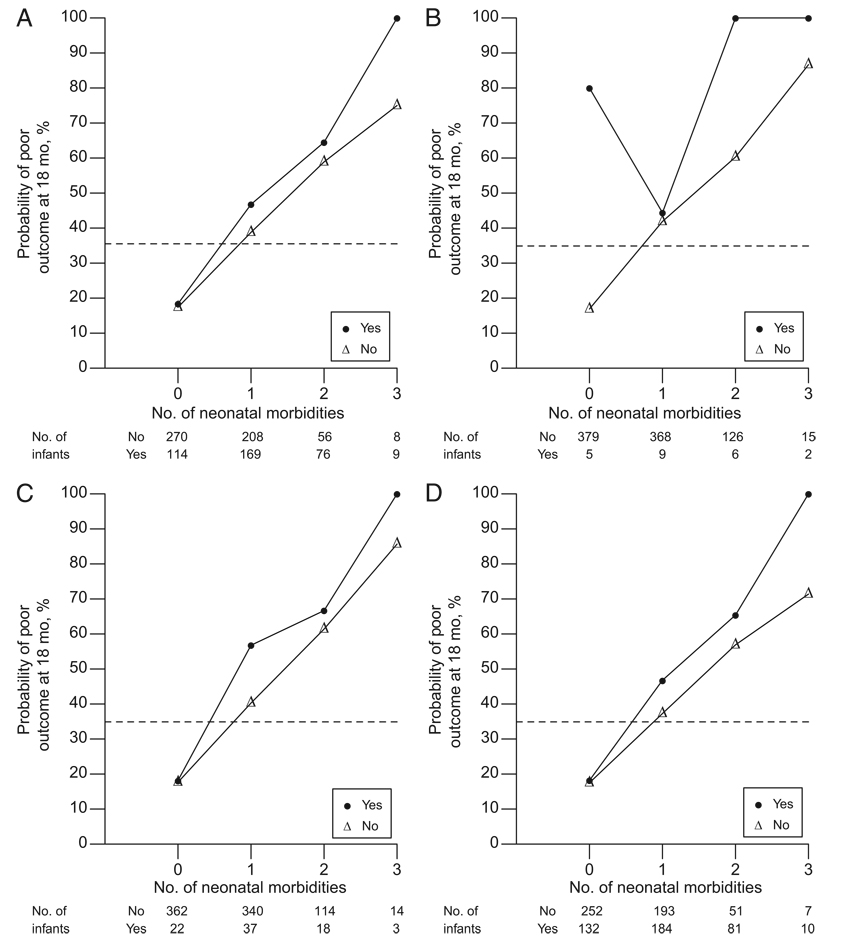
Objective: A count of 3 neonatal morbidities (bronchopulmonary dysplasia, brain injury, and severe retinopathy of prematurity) strongly predict the risk of death or neurosensory impairment in extremely low birth weight infants who survive to 36 weeks' postmenstrual age. Neonatal infection has also been linked with later impairment. We examined whether the addition of infection to the count of 3 neonatal morbidities further improves the prediction of poor outcome.
Methods: We studied 944 infants who participated in the Trial of Indomethacin Prophylaxis in Preterms and survived to 36 weeks' postmenstrual age. Culture-proven sepsis, meningitis, and stage II or III necrotizing enterocolitis were recorded prospectively. We investigated the incremental prognostic importance of neonatal infection by adding terms for the different types of infection to a logistic model that already contained terms for the count of bronchopulmonary dysplasia, brain injury, and severe retinopathy. Poor outcome at 18 months of age was death or survival with 1 or more of the following: cerebral palsy, cognitive delay, severe hearing loss, and bilateral blindness.
Results: There were 414 (44%) infants with at least 1 episode of infection or necrotizing enterocolitis. Meningitis and the presence of any type of infection added independent prognostic information to the morbidity-count model. The odds ratio associated with infection or necrotizing enterocolitis in this model was 50% smaller than the odds ratio associated with each count of the other 3 neonatal morbidities. Meningitis was rare and occurred in 22 (2.3%) of 944 infants.
Conclusions: In this cohort of extremely low birth weight infants who survived to 36 weeks' postmenstrual age, neonatal infection increased the risk of a late death or survival with neurosensory impairment. However, infection was a weaker predictor of poor outcome than bronchopulmonary dysplasia, brain injury, and severe retinopathy.
Trial registration: ClinicalTrials.gov NCT00009646.
Figures
References
-
- Vohr BR, Wright LL, Poole WK, McDonald SA. Neurodevelopmental outcomes of extremely low birth weight infants < 32 weeks’ gestation between 1993 and 1998. Pediatrics. 2005;116(3):635–643. - PubMed
-
- Wood NS, Marlow N, Costeloe K, Gibson AT, Wilkinson AR EPICure Study Group. Neurologic and developmental disability after extremely preterm birth. N Engl J Med. 2000;343(6):378–384. - PubMed
-
- Partridge JC, Martinez AM, Nishida H, et al. International comparison of care for very low birth weight infants: parents’ perceptions of counseling and decision-making. Pediatrics. 2005. Available at: www.pediatrics.org/cgi/content/full/116/2/e263. - PubMed
-
- Ambalavanan N, Baibergenova A, Carlo WA, et al. Early prediction of poor outcome in extremely low birth weight infants by classification tree analysis. J Pediatr. 2006;148(4):438–444. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10 HD27851/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- M01 RR 00070/RR/NCRR NIH HHS/United States
- M01 RR000997/RR/NCRR NIH HHS/United States
- U10 HD21373/HD/NICHD NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD21364/HD/NICHD NIH HHS/United States
- U10 HD34216/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- M01 RR 00997/RR/NCRR NIH HHS/United States
- U10 HD27880/HD/NICHD NIH HHS/United States
- UL1 TR001449/TR/NCATS NIH HHS/United States
- U10 HD27904/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD021397/HD/NICHD NIH HHS/United States
- UL1 TR000041/TR/NCATS NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- M01 RR000070/RR/NCRR NIH HHS/United States
- U10 HD21385/HD/NICHD NIH HHS/United States
- U10 HD027881/HD/NICHD NIH HHS/United States
- U10 HD27881/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
