

Design of combination angiotensin receptor blocker and angiotensin-converting enzyme inhibitor for treatment of diabetic nephropathy (VA NEPHRON-D)
- PMID: 19118120
- PMCID: PMC2637584
- DOI: 10.2215/CJN.03350708
Design of combination angiotensin receptor blocker and angiotensin-converting enzyme inhibitor for treatment of diabetic nephropathy (VA NEPHRON-D)
Abstract
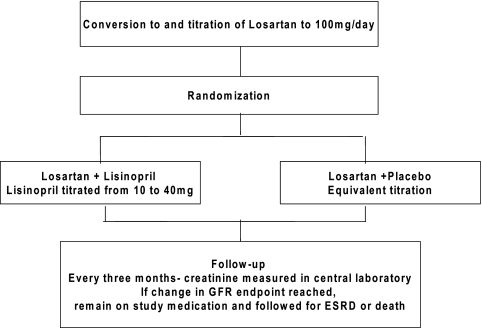
Both angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) can slow the progression of diabetic nephropathy. Even with ACEI or ARB treatment, the proportion of patients who progress to end-stage renal disease (ESRD) remains high. Interventions that achieve more complete blockade of the renin-angiotensin system, such as combination ACEI and ARB, might be beneficial. This approach may decrease progression of nondiabetic kidney disease. In diabetic nephropathy, combination therapy decreases proteinuria, but its effect in slowing progression is unknown. In addition, the potential for hyperkalemia may limit the utility of combined therapy in this population. VA NEPHRON-D is a randomized, double-blind, multicenter clinical trial to assess the effect of combination losartan and lisinopril, compared with losartan alone, on the progression of kidney disease in 1850 patients with diabetes and overt proteinuria. The primary endpoints are time to (1) reduction in estimated GFR (eGFR) of > 50% (if baseline < 60 ml/min/1.73 m(2)); (2) reduction in eGFR of 30 ml/min/1.73 m(2) (if baseline > or = 60 ml/min/1.73 m(2)); (3) progression to ESRD (need for dialysis, renal transplant, or eGFR < 15 ml/min/1.73 m(2)); or (4) death. The secondary endpoint is time to change in eGFR or ESRD. Tertiary endpoints are cardiovascular events, slope of change in eGFR, and change in albuminuria at 1 yr. Specific safety endpoints are serious hyperkalemia (potassium > 6 mEq/L, requiring admission, emergency room visit, or dialysis), all-cause mortality, and other serious adverse events. This paper discusses the design and key methodological issues that arose during the planning of the study.
Figures
References
-
- United States Renal Data System: USRDS 2003 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, in, edited by National Institutes of Health National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2003
-
- Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S: Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869, 2001 - PubMed
-
- Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E, Atkins RC, Rohde R, Raz I: Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 345: 851–860, 2001 - PubMed
-
- Azizi M, Menard J: Combined blockade of the renin-angiotensin system with angiotensin-converting enzyme inhibitors and angiotensin II type 1 receptor antagonists. Circulation 109: 2492–2499, 2004 - PubMed
-
- Nakao N, Yoshimura A, Morita H, Takada M, Kayano T, Ideura T: Combination treatment of angiotensin-II receptor blocker and angiotensin-converting-enzyme inhibitor in non-diabetic renal disease (COOPERATE): A randomised controlled trial. Lancet 361: 117–124, 2003 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
