

Improvements in orthostatic instability with stand locomotor training in individuals with spinal cord injury
- PMID: 19118454
- PMCID: PMC2729458
- DOI: 10.1089/neu.2008.0572
Improvements in orthostatic instability with stand locomotor training in individuals with spinal cord injury
Abstract
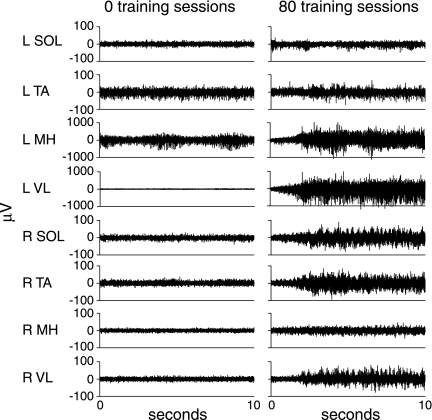
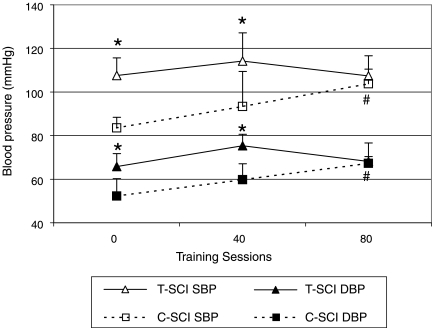
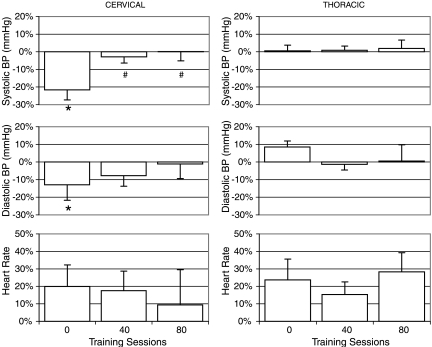
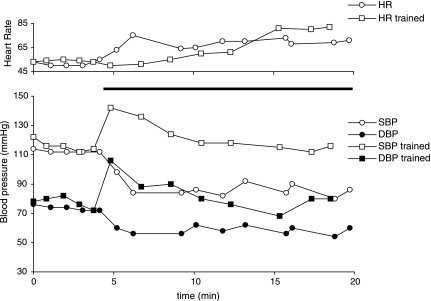
Prospective assessment of cardiovascular control in individuals with spinal cord injury (SCI) in response to active stand training. Cardiovascular parameters were measured at rest and in response to orthostatic challenge before and after training in individuals with clinically complete SCI. The goal of this study was to evaluate the effect of active stand training on arterial blood pressure and heart rate and changes in response to orthostatic stress in individuals with SCI. Measurements were obtained in individuals with SCI (n=8) prior to and after 40 and 80 sessions of the standing component of a locomotor training intervention (stand LT). During standing, all participants wore a harness and were suspended by an overhead, pneumatic body weight support (BWS) system over a treadmill. Trainers provided manual facilitation as necessary at the trunk and legs. All individuals were able to bear more weight on their legs after the stand LT training. Resting arterial blood pressure significantly increased in individuals with cervical SCI after 80 training sessions. At the end of the training period, resting systolic blood pressure (BP) in individuals with cervical SCI in a seated position, increased by 24% (from 84 +/- 5 to 104 +/- 7 mmHg). Furthermore, orthostatic hypotension present in response to standing prior to training (decrease in systolic BP of 24 +/- 14 mmHg) was not evident (decrease in systolic BP of 0 +/- 11 mmHg) after 80 sessions of stand LT. Hemodynamic parameters of individuals with thoracic SCI were relatively stable prior to training and not significantly different after 80 sessions of stand LT. Improvements in resting arterial blood pressure and responses to orthostatic stress in individuals with clinically complete cervical SCI occurred following intensive stand LT training. These results may be attributed to repetitive neuromuscular activation of the legs from loading and/or conditioning of cardiovascular responses from repetitively assuming an upright posture.
Figures
References
-
- Barbeau H. Locomotor training in neurorehabilitation: emerging rehabilitation concepts. Neurorehabil. Neural Repair. 2003;17:3–11. - PubMed
-
- Barbeau H. Norman K. Fung J. Visintin M. Ladouceur M. Does neurorehabilitation play a role in the recovery of walking in neurological populations? Ann. N. Y. Acad. Sci. 1998;860:377–392. - PubMed
-
- Barbeau H. Visintin M. Optimal outcomes obtained with body-weight support combined with treadmill training in stroke subjects. Arch. Phys. Med. Rehabil. 2003;84:1458–1465. - PubMed
-
- Barbeau H. Fung J. The role of rehabilitation in the recovery of walking in the neurological population. Curr. Opin. Neurol. 2001;14:735–740. - PubMed
-
- Barber D.B. Rogers S.J. Fredrickson M.D. Able A.C. Midodrine hydrochloride and the treatment of orthostatic hypotension in tetraplegia: two cases and a review of the literature. Spinal Cord. 2000;38:109–111. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
