

Revisiting rose: comparing the benefits and costs of population-wide and targeted interventions
- PMID: 19120981
- PMCID: PMC2614696
- DOI: 10.1111/j.1468-0009.2008.00535.x
Revisiting rose: comparing the benefits and costs of population-wide and targeted interventions
Abstract
Context: Geoffrey Rose's two principal approaches to public health intervention are (1) targeted strategies focusing on individuals at a personal increased risk of disease and (2) population-wide approaches focusing on the whole population. Beyond his discussion of the strengths and weaknesses of these approaches, there is no empiric work examining the conditions under which one of these approaches may be better than the other.
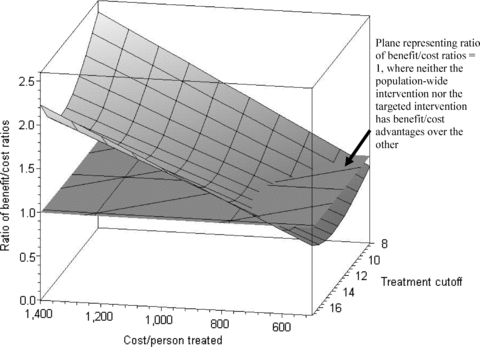
Methods: This article uses mathematical simulations to model the benefits and costs of the two approaches, varying the cut points for treatment, effect magnitudes, and costs of the interventions. These techniques then were applied to the specific example of an intervention on blood pressure to reduce cardiovascular disease.
Findings: In the general simulation (using an inverse logit risk curve), lower costs of intervention, treating people with risk factor values at or above where the slope on the risk curve is at its steepest (for targeted interventions), and interventions with larger effects on reducing the risk factor (for population-wide interventions) provided benefit/cost advantages. In the specific blood pressure intervention example, lower-cost population-wide interventions had better benefit/cost ratios, but some targeted treatments with lower cutoffs prevented more absolute cases of disease.
Conclusions: These simulations empirically evaluate some of Rose's original arguments. They can be replicated for particular interventions being considered and may be useful in helping public health decision makers assess potential intervention strategies.
Figures



References
-
- Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, Bray GA, Vogt TM, Cutler JA, Windhauser MM, Lin PH, Karanja N. A Clinical Trial of the Effects of Dietary Patterns on Blood Pressure. DASH Collaborative Research Group. New England Journal of Medicine. 1997;336:1117–24. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJ. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 Report. Journal of the American Medical Association. 2003;289:2560–72. - PubMed
-
- Diez Roux AV. The Study of Group-Level Factors in Epidemiology: Rethinking Variables, Study Designs, and Analytical Approaches. Epidemiologic Reviews. 2004;26:104–11. - PubMed
-
- Duncan C, Jones K, Moon G. Context, Composition and Heterogeneity: Using Multilevel Models in Health Research. Social Science and Medicine. 1998;46:97–117. - PubMed
-
- Kannel WB, McGee D, Gordon T. A General Cardiovascular Risk Profile: The Framingham Study. American Journal of Cardiology. 1976;38:46–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
