

Differential use of warfarin for secondary stroke prevention in patients with various types of atrial fibrillation
- PMID: 19121441
- PMCID: PMC3086549
- DOI: 10.1016/j.amjcard.2008.08.062
Differential use of warfarin for secondary stroke prevention in patients with various types of atrial fibrillation
Abstract
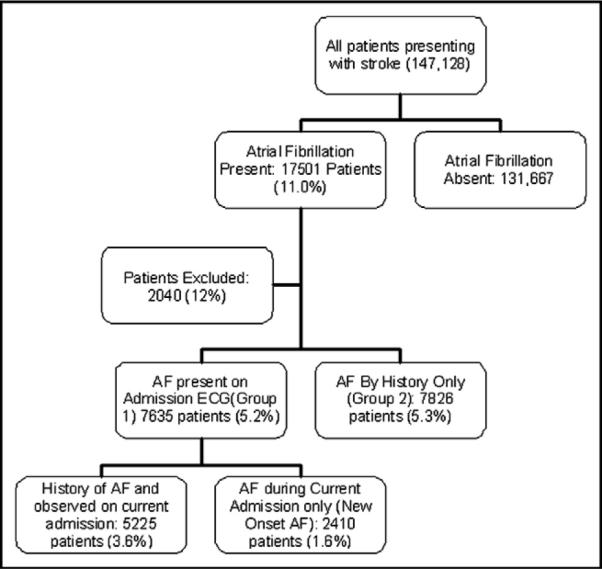
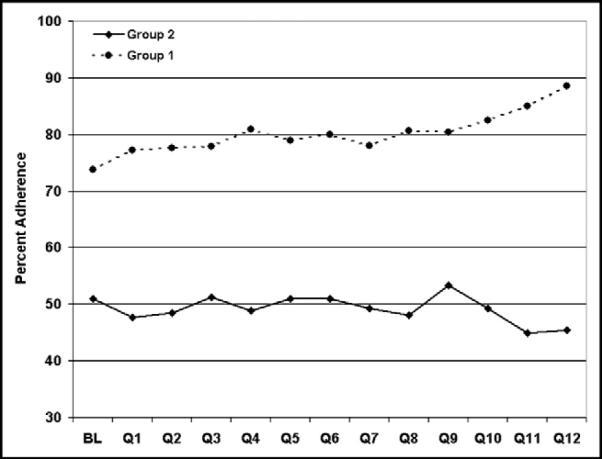
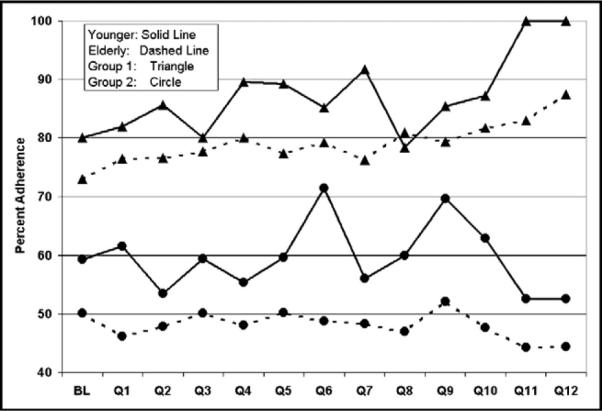
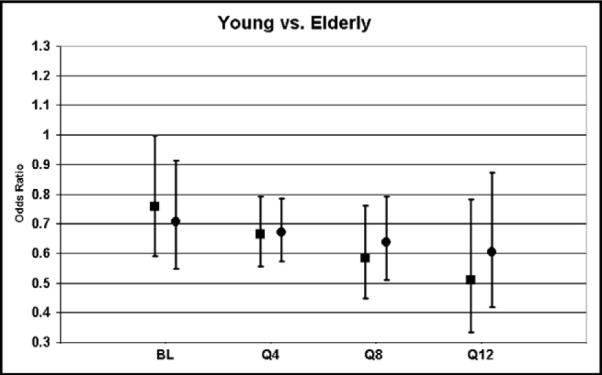
Anticoagulation therapy significantly reduces the incidence of thromboembolic events in patients with atrial fibrillation (AF), and warfarin therapy at discharge is a class I-indicated drug in patients with ischemic stroke with persistent or paroxysmal AF without contraindications. The aim was to determine whether participation in the Get With The Guidelines-Stroke (GWTG-S) quality improvement program would be associated with improved adherence to anticoagulation guidelines for patients with all types of AF. Adherence to warfarin treatment at hospital discharge was assessed in eligible patients with AF who presented with stroke or transient ischemic attack, based on type of AF. Of patients with stroke, 10.5% presented with some form of AF. When AF was documented using electrocardiography or telemetry (ECG) during the present admission, eligible patients were more likely to receive warfarin compared with patients for whom AF was reported using medical history only (78.8% vs 49.4%; p<0.0001). Improvement after GWTG-S participation in warfarin use was observed in patients with ECG-documented AF (73.8% at baseline vs 88.5% after the intervention; p<0.0001), but not patients using history only. Women and elderly patients were less likely to receive warfarin, and these gaps in treatment did not narrow during the quality improvement program for patients with ECG-documented AF and those with history only. In conclusion, anticoagulation for stroke prevention was underused in general for patients with AF, even in such high-risk groups as patients with stroke. GWTG-S was associated with improved adherence for patients with ECG-documented AF, but patients with a history of AF alone were largely untreated.
Figures
References
-
- Roe MT. Success stories: how hospitals are improving care. Am Heart J. 2004;148(suppl):S52–S55. - PubMed
-
- LaBresh KA, Reeves MJ, Frankel MR, Albright D, Schwamm LH. Hospital treatment of patients with ischemic stroke or transient ischemic attack using the “Get With The Guidelines” program. Arch Intern Med. 2008;168:411–417. - PubMed
-
- Hart RG, Pearce LA, Rothbart RM, McAnulty JH, Asinger RW, Halperin JL. Stroke with intermittent atrial fibrillation: incidence and predictors during aspirin therapy. Stroke Prevention in Atrial Fibrillation Investigators. J Am Coll Cardiol. 2000;35:183–187. - PubMed
-
- Atrial Fibrillation, Aspirin, Anticoagulation Study. Boston Area Anticoagulation Trial for Atrial Fibrillation Study. Canadian Atrial Fibrillation Anticoagulation Study. Stroke Prevention in Atrial Fibrillation Study. Veterans Affairs Stroke Prevention in Nonrheumatic Atrial Fibrillation Study Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994;154:1449–1457. - PubMed
-
- Marcu CB, Ghantous AE, Caracciolo EA, Donohue TJ. Patterns of anticoagulation in patients hospitalized with atrial fibrillation: warfarin is underused in paroxysmal atrial fibrillation. Conn Med. 2003;67:595–598. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
