

Delayed internal fixation of femoral shaft fracture reduces mortality among patients with multisystem trauma
- PMID: 19122073
- PMCID: PMC2663326
- DOI: 10.2106/JBJS.H.00338
Delayed internal fixation of femoral shaft fracture reduces mortality among patients with multisystem trauma
Abstract
Background: Fractures of the femoral shaft are common and have potentially serious consequences in patients with multiple injuries. The appropriate timing of fracture repair is controversial. The purpose of the present study was to assess the effect of timing of internal fixation on mortality in patients with multisystem trauma.
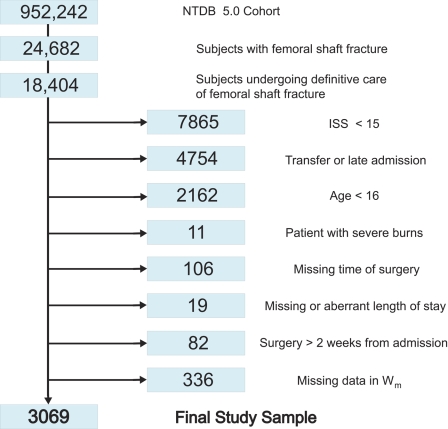
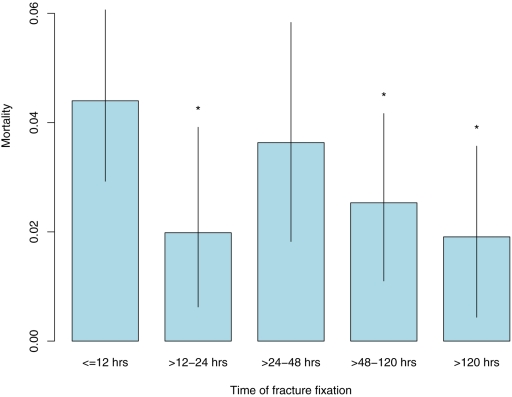
Methods: We performed a retrospective cohort study with use of data from public and private trauma centers throughout the United States that were reported to the National Trauma Data Bank (version 5.0 for 2000 through 2004). The study included 3069 patients with multisystem trauma (Injury Severity Score, > or =15) who underwent internal fixation of a femoral shaft fracture. The time to treatment was defined in categories as the time from admission to internal fixation: t(0) (twelve hours or less), t(1) (more than twelve hours to twenty-four hours), t(2) (more than twenty-four hours to forty-eight hours), t(3) (more than forty-eight hours to 120 hours), and t(4) (more than 120 hours). The relative risk of in-hospital mortality when the four later periods were compared with the earliest one was estimated with inverse probability of treatment-weighted analysis. Subgroups with serious head or neck, chest, abdominal, and additional extremity injury were investigated.
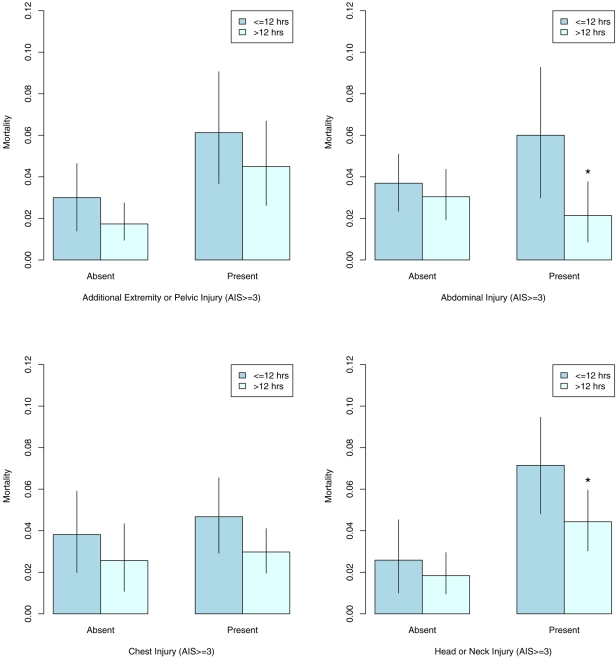
Results: When compared with that during the first twelve hours after admission, the estimated mortality risk was significantly lower in three time categories: t(1) (relative risk, 0.45; 95% confidence interval, 0.15 to 0.98; p = 0.03), t(3) (relative risk, 0.58; 95% confidence interval, 0.28 to 0.93; p = 0.03), and t(4) (relative risk, 0.43; 95% confidence interval, 0.10 to 0.94; p = 0.03). Patients with serious abdominal trauma (Abbreviated Injury Score, > or =3) experienced the greatest benefit from a delay of internal fixation beyond twelve hours (relative risk, 0.82 [95% confidence interval, 0.54 to 1.35] for patients with an Abbreviated Injury Score of <3, compared with 0.36 [95% confidence interval, 0.13 to 0.87] for those with an Abbreviated Injury Score of > or =3) (p value for effect modification, 0.09).
Conclusions: Delayed repair of femoral shaft fracture beyond twelve hours in patients with multisystem trauma, which may allow time for appropriate resuscitation, reduces mortality by approximately 50%. Patients with serious abdominal injury benefit most from delayed treatment. These results support delaying definitive treatment of long-bone injuries in patients with multisystem trauma as a means of so-called damage-control in order to reduce adverse outcomes.
Figures
References
-
- Riska EB, von Bonsdorff H, Hakkinen S, Jaroma H, Kiviluoto O, Paavilainen T. Prevention of fat embolism by early internal fixation of fractures in patients with multiple injuries. Injury. 1976;8:110-6. - PubMed
-
- Goris RJ, Gimbrere JS, van Niekerk JL, Schoots FJ, Booy LH. Early osteosynthesis and prophylactic mechanical ventilation in the multitrauma patient. J Trauma. 1982;22:895-903. - PubMed
-
- Johnson KD, Cadambi A, Seibert GB. Incidence of adult respiratory distress syndrome in patients with multiple musculoskeletal injuries: effect of early operative stabilization of fractures. J Trauma. 1985;25:375-84. - PubMed
-
- Bosse MJ, MacKenzie EJ, Riemer BL, Brumback RJ, McCarthy ML, Burgess AR, Gens DR, Yasui Y. Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated either with intramedullary nailing with reaming or with a plate. A comparative study. J Bone Joint Surg Am. 1997;79:799-809. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
