

Can UGT1A1 genotyping reduce morbidity and mortality in patients with metastatic colorectal cancer treated with irinotecan? An evidence-based review
- PMID: 19125129
- PMCID: PMC2743611
- DOI: 10.1097/GIM.0b013e31818efd77
Can UGT1A1 genotyping reduce morbidity and mortality in patients with metastatic colorectal cancer treated with irinotecan? An evidence-based review
Abstract
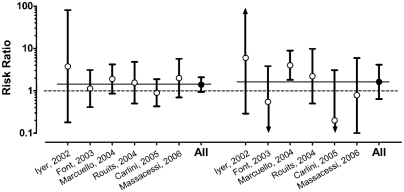
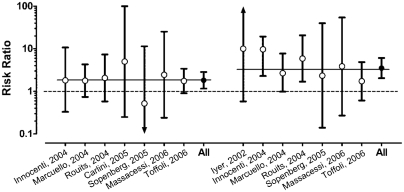
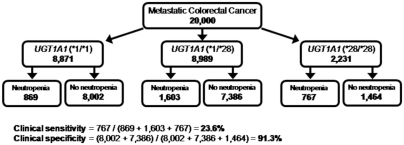
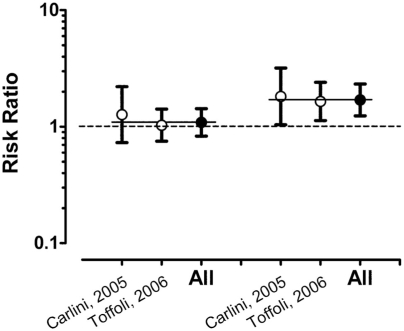
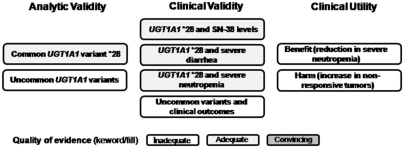
This evidence-based review addresses the question of whether testing for UGT1A1 mutations in patients with metastatic colorectal cancer treated with irinotecan leads to improvement in outcomes (e.g., irinotecan toxicity, response to treatment, morbidity, and mortality), when compared with no testing. No studies were identified that addressed this question directly. The quality of evidence on the analytic validity of current UGT1A1 genetic testing methods is adequate (scale: convincing, adequate, inadequate), with available data indicating that both analytic sensitivity and specificity for the common genotypes are high. For clinical validity, the quality of evidence is adequate for studies reporting concentration of the active form of irinotecan (SN-38), presence of severe diarrhea, and presence of severe neutropenia stratified by UGT1A1 common genotypes. The strongest association for a clinical endpoint is for severe neutropenia. Patients homozygous for the *28 allele are 3.5 times more likely to develop severe neutropenia compared with individuals with the wild genotype (risk ratio 3.51; 95% confidence interval 2.03-6.07). The proposed clinical utility of UGT1A1 genotyping would be derived from a reduction in drug-related adverse reactions (benefits) while at the same time avoiding declines in tumor response rate and increases in morbidity/mortality (harms). At least three treatment options for reducing this increased risk have been suggested: modification of the irinotecan regime (e.g., reduce initial dose), use of other drugs, and/or pretreatment with colony-stimulating factors. However, we found no prospective studies that examined these options, particularly whether a reduced dose of irinotecan results in a reduced rate of adverse drug events. This is a major gap in knowledge. Although the quality of evidence on clinical utility is inadequate, two of three reviewed studies (and one published since our initial selection of studies for review) found that individuals homozygous for the *28 allele had improved survival. Three reviewed studies found statistically significant higher tumor response rates among individuals homozygous for the *28 allele. We found little or no direct evidence to assess the benefits and harms of modifying irinotecan regimens for patients with colorectal cancer based on their UGT1A1 genotype; however, results of our preliminary modeling of prevalence, acceptance, and effectiveness indicate that reducing the dose would need to be highly effective to have benefits outweigh harms. An alternative is to increase irinotecan dose among wild-type individuals to improve tumor response with minimal increases in adverse drug events. Given the large number of colorectal cancer cases diagnosed each year, a randomized controlled trial of the effects of irinotecan dose modifications in patients with colorectal cancer based on their UGT1A1 genotype is feasible and could clarify the tradeoffs between possible reductions in severe neutropenia and improved tumor response and/or survival in patients with various UGT1A1 genotypes.
Figures
References
-
- Centers for Disease Control and Prevention. Colorectal cancer: the importance of prevention and early detection (fact sheet) [Accessed July 18, 2008]. Available at: http://www.cdc.gov/cancer/colorectal/pdf/about2004.pdf.
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–130. - PubMed
-
- Wu X, Cokkinides V, Chen VW, et al. Associations of subsite-specific colorectal cancer incidence rates and stage of disease at diagnosis with county-level poverty, by race and sex. Cancer. 2006;107:1121–1127. - PubMed
-
- Pessino A, Sobrero A. Optimal treatment of metastatic colorectal cancer. Expert Rev Anticancer Ther. 2006;6:801–812. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
