

Lateral radiological evaluation of transarticular screw placement in the lower cervical spine
- PMID: 19130097
- PMCID: PMC2899426
- DOI: 10.1007/s00586-008-0861-0
Lateral radiological evaluation of transarticular screw placement in the lower cervical spine
Abstract
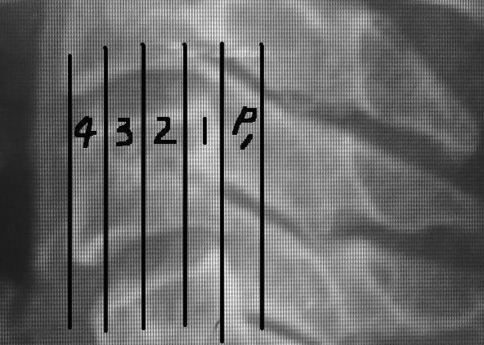
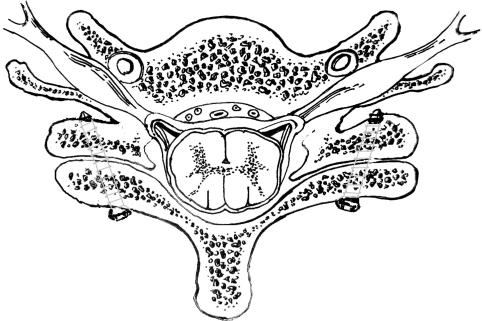
This study assessed the ideal district of lateral radiograph in evaluation of transarticular screw placement in the lower cervical spine. To assess the ideal zone of lateral radiographs in determining the safe or hazardous locations of the screw tips during transarticular screw implantation in the lower cervical spine. Transarticular screw in the lower cervical spine had been used as an alternative technique to achieve posterior cervical spine stability. Injury to the spinal nerves caused by transarticular screws which are too long must be identified quickly to minimize the neurologic complication. No previous radiological study regarding evaluation of the transarticular screw placement using lateral radiographs has been reported. Twelve cervical spines were removed from embalmed cadavers. Four transarticular screw placements with Dalcanto's technique under direct visualization, including placement of the screw tip staying the ventral cortex, 2, 4 and 6 mm over-penetration of the ventral cortex, were performed on each specimen. Following each placement, a lateral radiograph was taken. Each vertebral body was divided vertically into four equal zones, and another equal zone posterior to the posterior border of the vertebral body was defined as Zone pre-1. The numbers of screw tips seen in each zone were quantified for each placement. Partitions of chi (2) method was used to evaluate the ideal zone on lateral radiograph for transarticular screw insertion. At C34 and C45, no significant difference was found between Zone pre-1 and Zone 1 (chi(2) = 0.18, P > 0.50), while there was significant difference between Zones 1 and 2 (chi(2) = 73.6, P < 0.005), as well as Zones 2 and 3 (chi(2) = 13.2, P < 0.005). At C56 and C67, No significant difference was found between Zones 2 and 3 (chi(2) = 0.25, P > 0.50), while there was significant difference between Zone pre-1 and Zone 1 (chi(2) = 66.2, P < 0.005), as well as Zones 1 and 2 (chi(2) = 10.5, P < 0.005). Ideal screw tip positions on lateral radiograph for transarticular screw by Dalcanto's technique should be in Zone 1 at C34 and C45, in Zone pre-1 at C56 and C67. If the screw tip was in Zones 3 and 4, the safe rate will be decreased significantly and it might be too deep and be dangerous.
Figures





References
-
- Barrey C, Mertens P, Jund J et al (2005) Quantitative anatomic evaluation of cervical lateral mass fixation with a comparison of the Roy-Camille and the Magerl screw techniques. Spine 6:E140–E147 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
