Early decompressive craniectomy for neurotrauma: an institutional experience
- PMID: 19130336
- PMCID: PMC3413286
Early decompressive craniectomy for neurotrauma: an institutional experience
Abstract
Background: Neurotrauma centers have developed management protocols on the basis of evidence obtained from literature analysis and institutional experience. This article reviews our institutional experience in the management of severe traumatic brain injury (TBI) at Simòn Bolivar Hospital, the district trauma center for Bogotá's north zone.
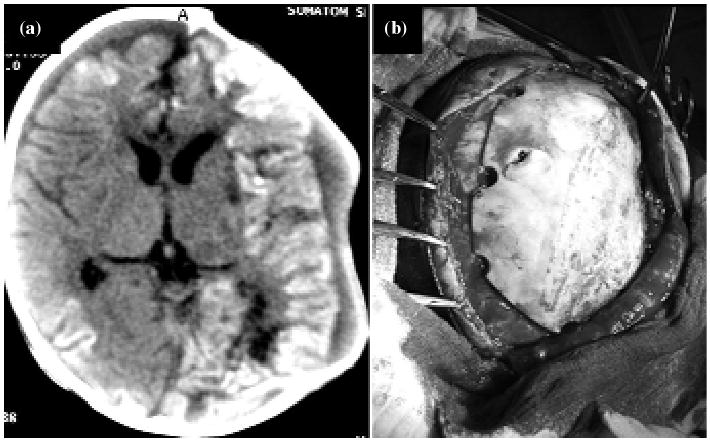
Methods: This is a case control study comparing a group of patients (n: 16) operated for severe TBI between January 2002 and July 2004 according to an institutional management protocol characterized by an early decompressive craniectomy (DC) approach versus a historical control group (n: 20) managed before the implementation of such protocol. Mortality and Glasgow Outcome Score (GOS) at 6 months were used as the main outcome variables.
Results: An early DC protocol implemented within 12 hours from injury in 16 patients with severe isolated TBI and a Marshall score between III or IV was associated with a lesser mortality than the conventional approach with ventriculostomy and Intensive Care Unit (ICU) management alone. The GOS was significantly better in the DC group (p=0.0002) than in the control group.
Conclusion: The use of an early DC protocol for severe TBI patients (Glasgow Coma Scale <9) had a significantly improved outcome compared with the conventional approach with ventriculostomy and ICU management in Simòn Bolivar Hospital in Bogotá, Colombia.
Figures

References
-
- The Brain Trauma Foundation. The American Association of Neurological Surgeons. The Joint Section on Neurotrauma and Critical Care. Trauma systems. J Neurotrauma. 2000;17:457–62. - PubMed
-
- Guidelines for the management of severe head injury. Introduction. J Neurotrauma. 1996;13:643–5. - PubMed
-
- Brain Trauma Foundation: Guidelines for surgical management of traumatic brain injury. BTF (New York), Neurosurgery. 2006;58:S2–S120.
-
- Gabriel EJ, Ghajar J, Jagoda A, Pons PT, Scalea T, Walters BC, Brain Trauma Foundation Guidelines for prehospital management of traumatic brain injury. J Neurotrauma. 2002;19:111–74. - PubMed
-
- Brain Trauma Foundation, Society of Critical Care Medicine, American Association of Neurological Surgeons, Join Sections of Pediatrics and Neurotrauma, American Academy of Pediatrics, World Federation of Pediatric Intensive and Critical Care Societies, American College of Emergency Physicians, Congress of Neurological Surgeons. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Pediatr Crit Care Med. 2003;4:1–72.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources