

Survival after hepatic resection of colorectal cancer metastases: a national experience
- PMID: 19130462
- PMCID: PMC2740982
- DOI: 10.1002/cncr.24081
Survival after hepatic resection of colorectal cancer metastases: a national experience
Abstract
Background: Most estimates of short- and long-term survival after hepatic resection of colorectal cancer metastases are derived from surgical case series. For the current report, the authors used Medicare data to investigate operative mortality and long-term survival in a national sample and examined the factors associated with survival.
Methods: Data were analyzed from Medicare enrollees (age >or=65 years) who were admitted to hospital between January 1, 2000 and December 31, 2004 with a primary diagnosis of colorectal cancer with resection. The sample was restricted to patients who subsequently underwent hepatic resection for liver metastases. The Medicare Denominator File was used to determine operative mortality and long-term survival and the factors that were associated with those outcomes.
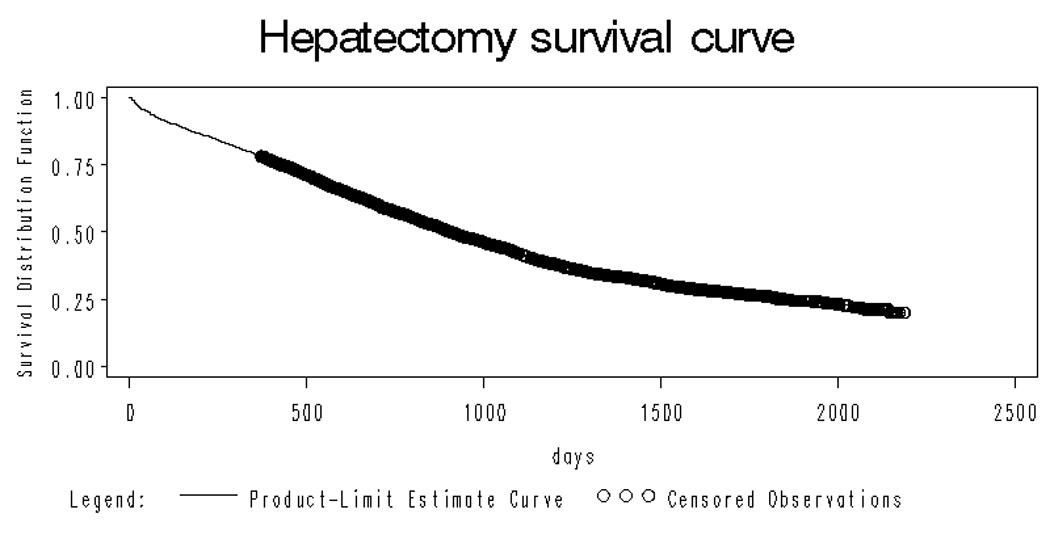
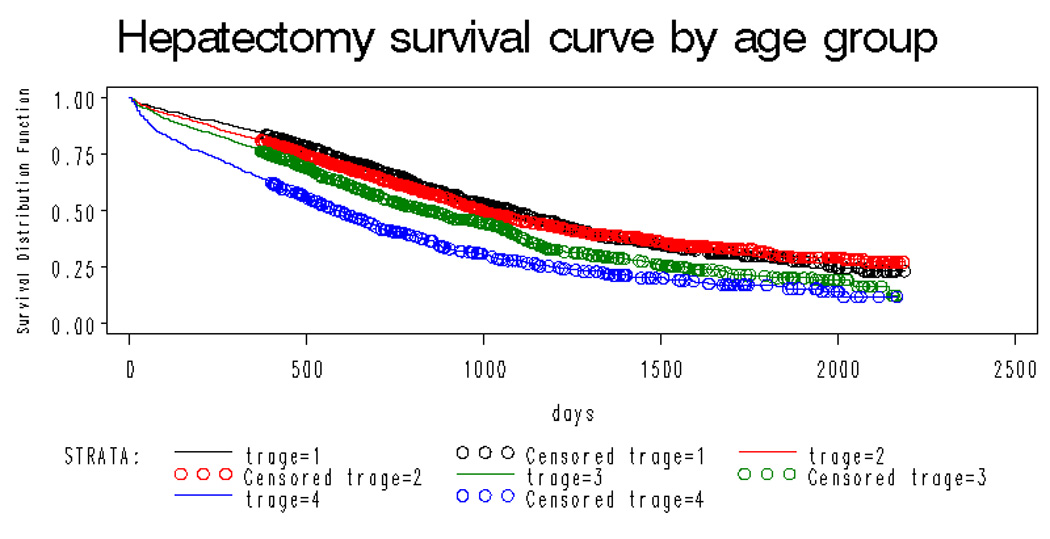
Results: Of the 306,061 Medicare beneficiaries who were diagnosed with colorectal cancer, 3957 patients were identified who underwent hepatic resection for liver metastases. The crude 30-day and 90-day mortality rates were 4% and 8.2%, respectively, and the 5-year survival rate was 25.5%. Advancing age (hazards ratio [HR], 1.83; 95% confidence interval [95% CI], 1.32-2.53 for age >or=80 years vs ages 65-69 years), comorbid disease (HR, 1.40; 95% CI, 1.06-1.85 for Charlson >or=5 vs Charlson 0), and synchronous colon/hepatic resection (HR, 2.46; 95% CI, 1.89-3.20 for synchronous vs metachronous resection) were associated with worse 90-day mortality. Similarly, long-term mortality was associated with age (HR, 1.36; 95% CI, 1.18-1.56), comorbid disease (HR, 1.51; 95% CI, 1.36-1.69), and synchronous colon/hepatic resection (HR, 1.37; 95% CI, 1.24-1.51 for synchronous vs metachronous resection).
Conclusions: In this national study, short- and long-term survival was worse than that reported in surgical case series. Subgroups at high risk for worse outcomes include the extreme elderly and those undergoing synchronous colon and hepatic resection.
(c) 2009 American Cancer Society.
Figures
Comment in
-
The patient behind the code, the care behind the patient.Cancer. 2009 Feb 15;115(4):702-3. doi: 10.1002/cncr.24095. Cancer. 2009. PMID: 19127555 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007 Jan–Feb;57(1):43–66. - PubMed
-
- Saltz LB, Cox JV, Blanke C, et al. Irinotecan Study Group. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. N Engl J Med. 2000 Sep 28;343(13):905–914. - PubMed
-
- Douillard JY, Cunningham D, Roth AD, et al. Irinotecan combined with fluorouracil compared with fluorouracil alone as first-line treatment for metastatic colorectal cancer: a multicentre randomised trial. Lancet. 2000 Mar 25;355(9209):1041–1047. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
