

Operations and pelvic muscle training in the management of apical support loss (OPTIMAL) trial: design and methods
- PMID: 19130903
- PMCID: PMC2646798
- DOI: 10.1016/j.cct.2008.12.001
Operations and pelvic muscle training in the management of apical support loss (OPTIMAL) trial: design and methods
Abstract
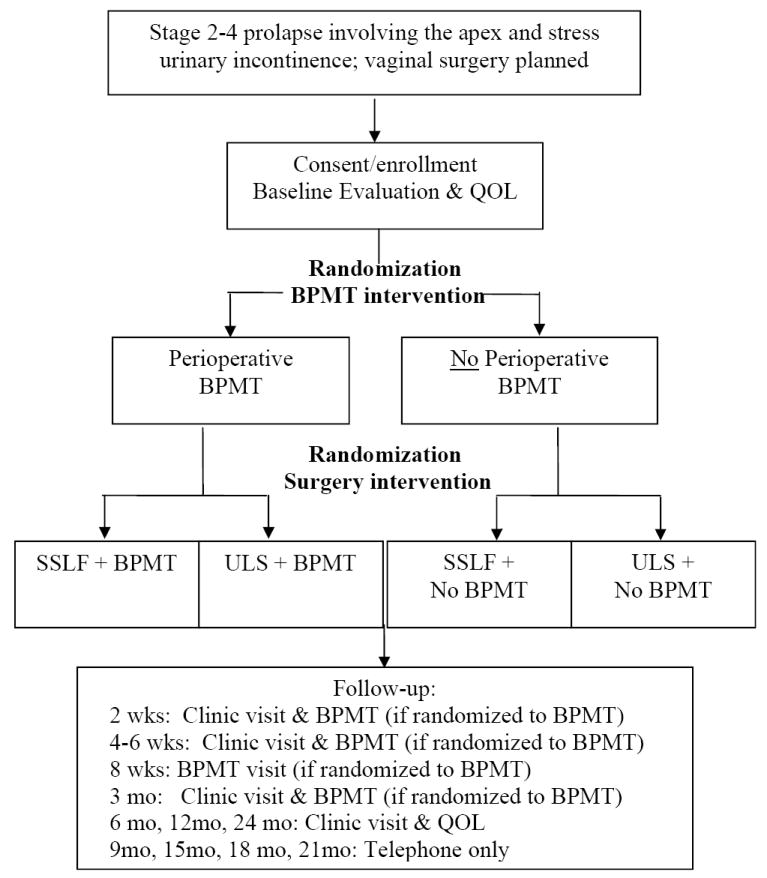
The primary aims of this trial are: 1) to compare surgical outcomes following sacrospinous ligament fixation to uterosacral vaginal vault suspension in women undergoing vaginal surgery for apical or uterine pelvic organ prolapse and stress urinary incontinence and 2) to examine the effects of a structured perioperative program consisting of behavioral techniques and pelvic floor muscle training compared to usual care. This trial is performed through the Pelvic Floor Disorders Network (PFDN), which is funded by National Institute of Child Health and Human Development. Subjects will be enrolled from hospitals associated with seven PFDN clinical centers across the United States. A centralized biostatistical coordinating center will oversee data collection and analysis. Two approaches will be investigated simultaneously using a 2x2 randomized factorial design: a surgical intervention (sacrospinous ligament fixation versus uterosacral vaginal vault suspension) and a perioperative behavioral intervention (behavioral and pelvic floor muscle training versus usual care). Surgeons have standardized essential components of each surgical procedure and have met specific standards of expertise. Providers of the behavioral intervention have undergone standardized training. Anatomic, functional, and health-related quality of life outcomes will be assessed using validated measures by researchers blinded to all randomization assignments. Cost-effectiveness analysis will be performed using prospectively collected data on health care costs and resource utilization. The primary surgical endpoint is a composite outcome defined by anatomic recurrence, recurrence of bothersome vaginal prolapse symptoms and/or retreatment and will be assessed 2 years after the index surgery. Endpoints for the behavioral intervention include both short-term (6-month) improvement in urinary symptoms and long-term (2-year) improvement in anatomic outcomes and prolapse symptoms. This article describes the rationale and design of this randomized trial, focusing on several key design features of potential interest to researchers in the field of female pelvic floor disorders and others conducting randomized surgical trials.
Trial registration: ClinicalTrials.gov NCT00597935.
Figures
References
-
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89:501–6. - PubMed
-
- Clark AL, Gregory T, Smith VJ, Edwards R. Epidemiologic evaluation of reoperation for surgically treated pelvic organ prolapse and urinary incontinence. Am J Obstet Gynecol. 2003;189:1261–7. - PubMed
-
- Brown JS, Waetjen LE, Subak LL, Thom DH, Van den Eeden S, Vittinghoff E. Pelvic organ prolapse surgery in the United States, 1997. Am J Obstet Gynecol. 2002;186:712–6. - PubMed
-
- Boyles SH, Weber AM, Meyn L. Procedures for pelvic organ prolapse in the United States, 1979-1997. Am J Obstet Gynecol. 2003;188:108–15. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10 HD041261/HD/NICHD NIH HHS/United States
- U01 HD041249/HD/NICHD NIH HHS/United States
- U10 HD41267/HD/NICHD NIH HHS/United States
- U10 HD054215/HD/NICHD NIH HHS/United States
- U10 HD054214/HD/NICHD NIH HHS/United States
- U10 HD54215/HD/NICHD NIH HHS/United States
- U10 HD41261/HD/NICHD NIH HHS/United States
- U10 HD041267/HD/NICHD NIH HHS/United States
- U10 HD054136/HD/NICHD NIH HHS/United States
- U10 HD054241/HD/NICHD NIH HHS/United States
- U10 HD041250/HD/NICHD NIH HHS/United States
- U10 HD54241/HD/NICHD NIH HHS/United States
- U10 HD54136/HD/NICHD NIH HHS/United States
- U10 HD41250/HD/NICHD NIH HHS/United States
- U10 HD54214/HD/NICHD NIH HHS/United States
- U01 HD41249/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
