

Clinical effectiveness of beta-blockers in heart failure: findings from the OPTIMIZE-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure) Registry
- PMID: 19130987
- PMCID: PMC3513266
- DOI: 10.1016/j.jacc.2008.09.031
Clinical effectiveness of beta-blockers in heart failure: findings from the OPTIMIZE-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure) Registry
Abstract
Objectives: We sought to examine associations between initiation of beta-blocker therapy and outcomes among elderly patients hospitalized for heart failure.
Background: Beta-blockers are guideline-recommended therapy for heart failure, but their clinical effectiveness is not well understood, especially in elderly patients.
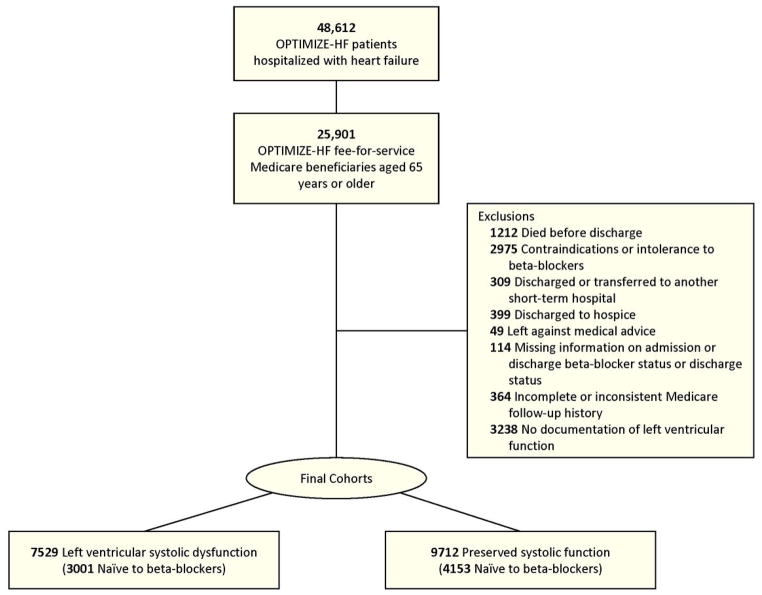
Methods: We merged Medicare claims data with OPTIMIZE-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients With Heart Failure) records to examine long-term outcomes of eligible patients newly initiated on beta-blocker therapy. We used inverse probability-weighted Cox proportional hazards models to determine the relationships among treatment and mortality, rehospitalization, and a combined mortality-rehospitalization end point.
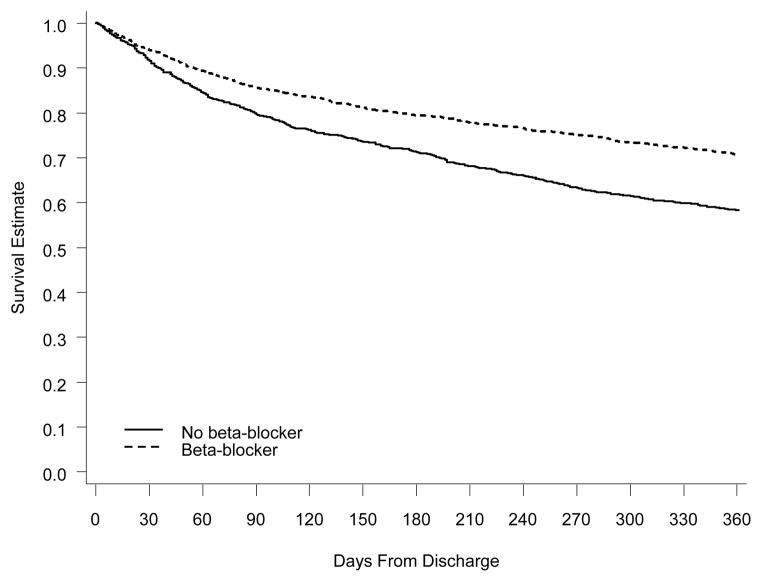
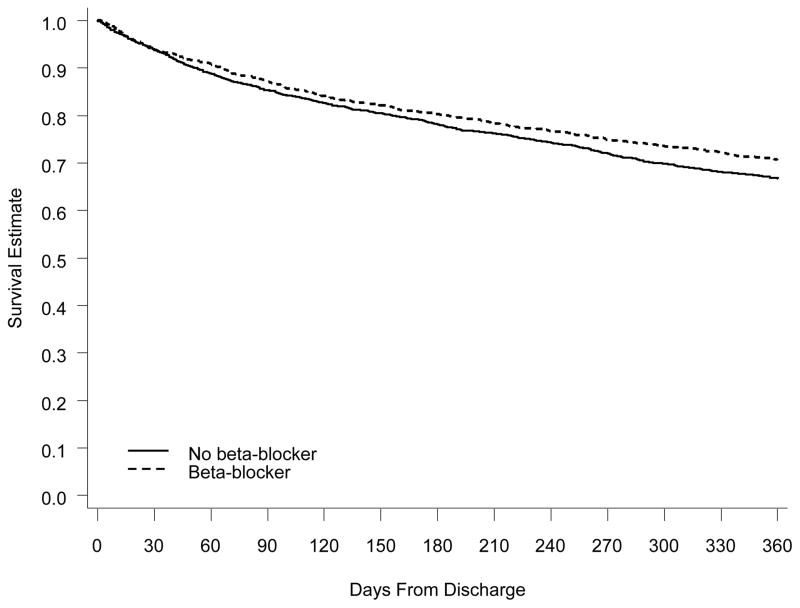
Results: Observed 1-year mortality was 33%, and all-cause rehospitalization was 64%. Among 7,154 patients hospitalized with heart failure and eligible for beta-blockers, 3,421 (49%) were newly initiated on beta-blocker therapy. Among patients with left ventricular systolic dysfunction (LVSD) (n = 3,001), beta-blockers were associated with adjusted hazard ratios of 0.77 (95% confidence interval [CI]: 0.68 to 0.87) for mortality, 0.89 (95% CI: 0.80 to 0.99) for rehospitalization, and 0.87 (95% CI: 0.79 to 0.96) for mortality-rehospitalization. Among patients with preserved systolic function (n = 4,153), beta-blockers were associated with adjusted hazard ratios of 0.94 (95% CI: 0.84 to 1.07) for mortality, 0.98 (95% CI: 0.90 to 1.06) for rehospitalization, and 0.98 (95% CI: 0.91 to 1.06) for mortality-rehospitalization.
Conclusions: In elderly patients hospitalized with heart failure and LVSD, incident beta-blocker use was clinically effective and independently associated with lower risks of death and rehospitalization. Patients with preserved systolic function had poor outcomes, and beta-blockers did not significantly influence the mortality and rehospitalization risks for these patients.
Figures
Comment in
-
Beta-blockers in elderly patients with heart failure ready for prime time?J Am Coll Cardiol. 2009 Dec 1;54(23):2202. doi: 10.1016/j.jacc.2009.02.093. J Am Coll Cardiol. 2009. PMID: 19942096 No abstract available.
References
-
- Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–146. - PubMed
-
- Krumholz HM, Parent EM, Tu N, et al. Readmission after hospitalization for congestive heart failure among Medicare beneficiaries. Arch Intern Med. 1997;157:99–104. - PubMed
-
- Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154–235. - PubMed
-
- Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF) Lancet. 1999;353:2001–7. - PubMed
-
- The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999;353:9–13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
