

Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: a Swedish prospective screening study in 39,821 newborns
- PMID: 19131383
- PMCID: PMC2627280
- DOI: 10.1136/bmj.a3037
Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: a Swedish prospective screening study in 39,821 newborns
Abstract
Objective: To evaluate the use of pulse oximetry to screen for early detection of life threatening congenital heart disease.
Design: Prospective screening study with a new generation pulse oximeter before discharge from well baby nurseries in West Götaland. Cohort study comparing the detection rate of duct dependent circulation in West Götaland with that in other regions not using pulse oximetry screening. Deaths at home with undetected duct dependent circulation were included.
Setting: All 5 maternity units in West Götaland and the supraregional referral centre for neonatal cardiac surgery.
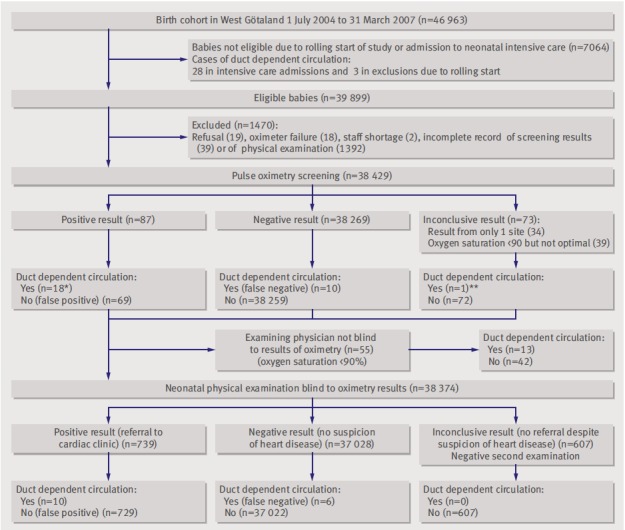
Participants: 39,821 screened babies born between 1 July 2004 and 31 March 2007. Total duct dependent circulation cohorts: West Götaland n=60, other referring regions n=100.
Main outcome measures: Sensitivity, specificity, positive and negative predictive values, and likelihood ratio for pulse oximetry screening and for neonatal physical examination alone.
Results: In West Götaland 29 babies in well baby nurseries had duct dependent circulation undetected before neonatal discharge examination. In 13 cases, pulse oximetry showed oxygen saturations <or=90%, and (in accordance with protocol) clinical staff were immediately told of the results. Of the remaining 16 cases, physical examination alone detected 10 (63%). Combining physical examination with pulse oximetry screening had a sensitivity of 24/29 (82.8% (95% CI 64.2% to 95.2%)) and detected 100% of the babies with duct dependent lung circulation. Five cases were missed (all with aortic arch obstruction). False positive rate with pulse oximetry was substantially lower than that with physical examination alone (69/39 821 (0.17%) v 729/38 413 (1.90%), P<0.0001), and 31/69 of the "false positive" cases with pulse oximetry had other pathology. Thus, referral of all cases with positive oximetry results for echocardiography resulted in only 2.3 echocardiograms with normal cardiac findings for every true positive case of duct dependent circulation. In the cohort study, the risk of leaving hospital with undiagnosed duct dependent circulation was 28/100 (28%) in other referring regions versus 5/60 (8%) in West Götaland (P=0.0025, relative risk 3.36 (95% CI 1.37 to 8.24)). In the other referring regions 11/25 (44%) of babies with transposition of the great arteries left hospital undiagnosed versus 0/18 in West Götaland (P=0.0010), and severe acidosis at diagnosis was more common (33/100 (33%) v 7/60 (12%), P=0.0025, relative risk 2.8 (1.3 to 6.0)). Excluding premature babies and Norwood surgery, babies discharged without diagnosis had higher mortality than those diagnosed in hospital (4/27 (18%) v 1/110 (0.9%), P=0.0054). No baby died from undiagnosed duct dependent circulation in West Götaland versus five babies from the other referring regions.
Conclusion: Introducing pulse oximetry screening before discharge improved total detection rate of duct dependent circulation to 92%. Such screening seems cost neutral in the short term, but the probable prevention of neurological morbidity and reduced need for preoperative neonatal intensive care suggest that such screening will be cost effective long term.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Neonatal screening for life threatening congenital heart disease.BMJ. 2009 Jan 8;338:a2663. doi: 10.1136/bmj.a2663. BMJ. 2009. PMID: 19131381 No abstract available.
-
Pulse oximetry before discharge from the nursery can increase detection of serious congenital heart disease.J Pediatr. 2009 Jul;155(1):147-8. doi: 10.1016/j.jpeds.2009.03.053. J Pediatr. 2009. PMID: 19559307 No abstract available.
References
-
- Mellander M, Sunnegardh J. Failure to diagnose critical heart malformations in newborns before discharge—an increasing problem? Acta Paediatr 2006;95:407-13. - PubMed
-
- Wren C, Reinhardt Z, Khawaja K. Twenty-year trends in diagnosis of life-threatening neonatal cardiovascular malformations. Arch Dis Child Fetal Neonatal Ed 2008;93:F33-5. - PubMed
-
- Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K, et al. Heart disease and stroke statistics--2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2007;115:e69-171. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical