

Use of Framingham risk score and new biomarkers to predict cardiovascular mortality in older people: population based observational cohort study
- PMID: 19131384
- PMCID: PMC2615548
- DOI: 10.1136/bmj.a3083
Use of Framingham risk score and new biomarkers to predict cardiovascular mortality in older people: population based observational cohort study
Abstract
Objectives: To investigate the performance of classic risk factors, and of some new biomarkers, in predicting cardiovascular mortality in very old people from the general population with no history of cardiovascular disease.
Design: The Leiden 85-plus Study (1997-2004) is an observational prospective cohort study with 5 years of follow-up.
Setting: General population of the city of Leiden, the Netherlands.
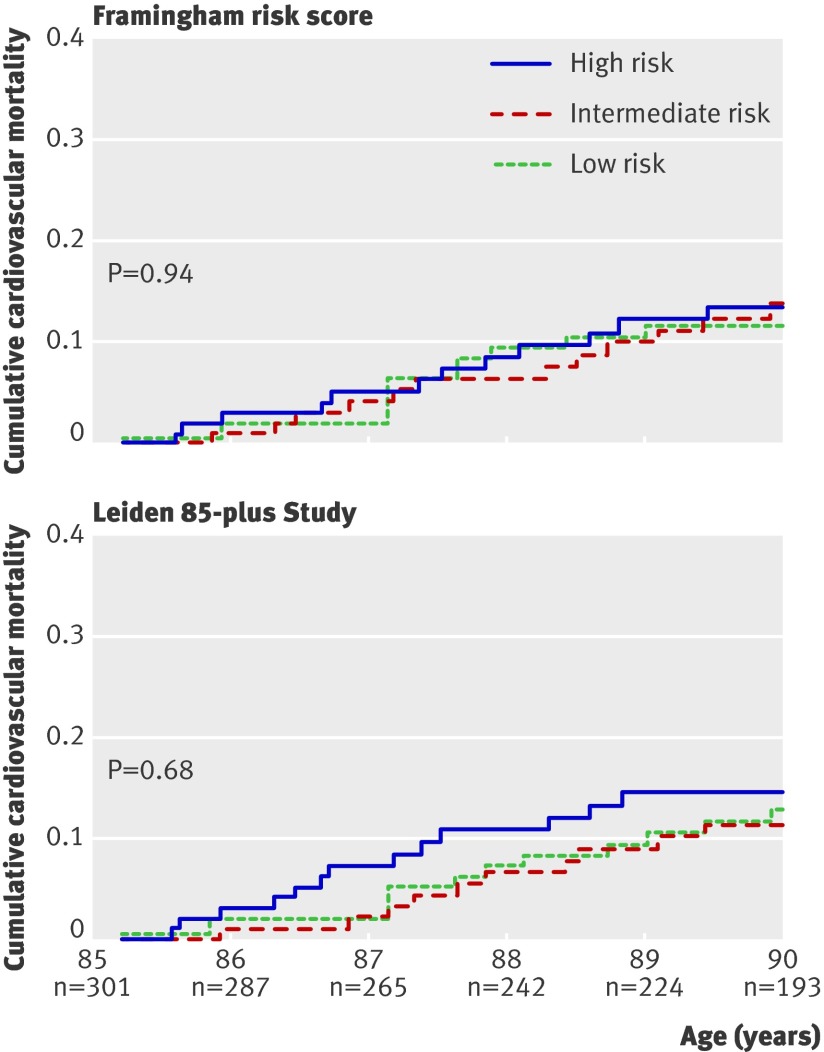
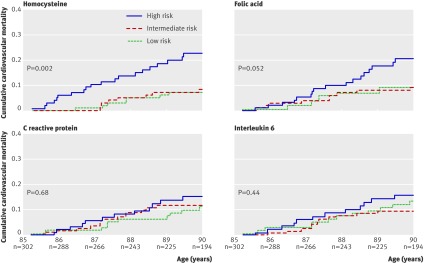
Participants: Population based sample of participants aged 85 years (215 women and 87 men) with no history of cardiovascular disease; no other exclusion criteria. Main measurements Cause specific mortality was registered during follow-up. All classic risk factors included in the Framingham risk score (sex, systolic blood pressure, total and high density lipoprotein cholesterol, diabetes mellitus, smoking and electrocardiogram based left ventricular hypertrophy), as well as plasma concentrations of the new biomarkers homocysteine, folic acid, C reactive protein, and interleukin 6, were assessed at baseline.
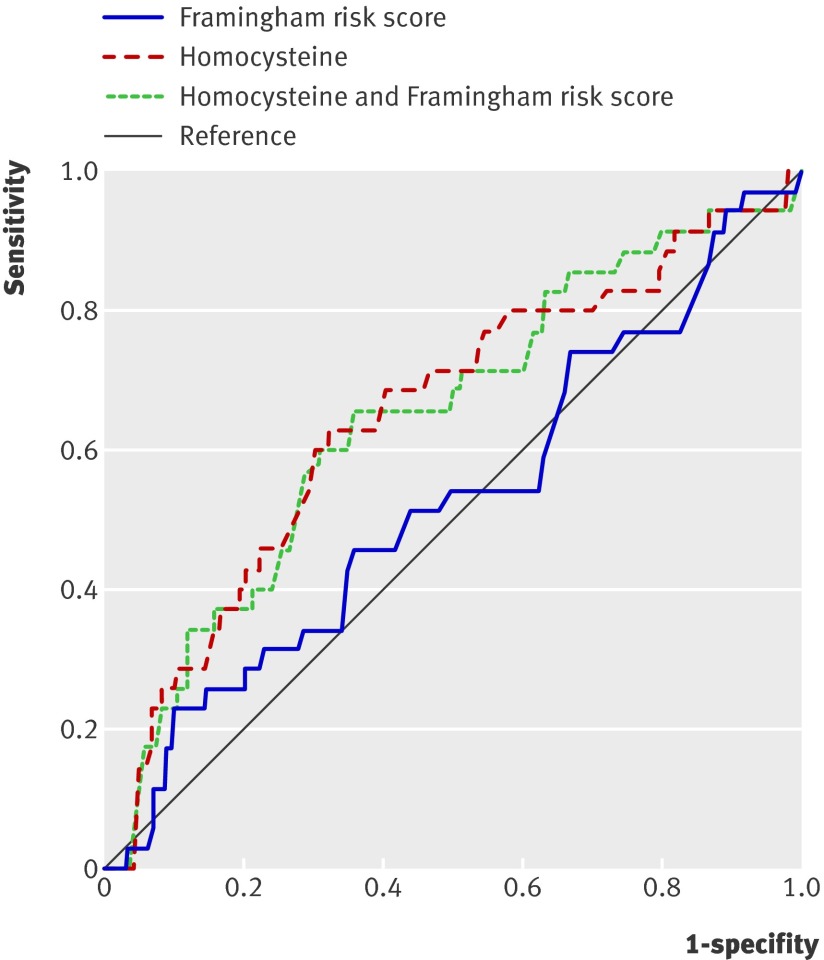
Results: During follow-up, 108 of the 302 participants died; 32% (35/108) of deaths were from cardiovascular causes. Classic risk factors did not predict cardiovascular mortality when used in the Framingham risk score (area under receiver operating characteristic curve 0.53, 95% confidence interval 0.42 to 0.63) or in a newly calibrated model (0.53, 0.43 to 0.64). Of the new biomarkers studied, homocysteine had most predictive power (0.65, 0.55 to 0.75). Entering any additional risk factor or combination of factors into the homocysteine prediction model did not increase its discriminative power.
Conclusions: In very old people from the general population with no history of cardiovascular disease, concentrations of homocysteine alone can accurately identify those at high risk of cardiovascular mortality, whereas classic risk factors included in the Framingham risk score do not. These preliminary findings warrant validation in a separate cohort.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- McDermott MM. The international pandemic of chronic cardiovascular disease. JAMA 2007;297:1253-5. - PubMed
-
- Petersen S, Peto V, Rayner M, Leal J, Luengo-Fernandez R, Gray A. European cardiovascular disease statistics. London: British Heart Foundation, 2005.
-
- Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K, et al. Heart disease and stroke statistics—2007 update: a report from the American Heart Association statistics committee and stroke statistics subcommittee. Circulation 2007;115:e69-171. - PubMed
-
- Mulrow CD, Cornell JA, Herrera CR, Kadri A, Farnett L, Aguilar C. Hypertension in the elderly. Implications and generalizability of randomized trials. JAMA 1994;272:1932-8. - PubMed
-
- Kannel WB. Cardiovascular disease preventive measures for the older patient: An epidemiologic perspective. Am J Geriatr Cardiol 2006;15:382-8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials