

Clinical and angiographic results of coiling of 196 very small (< or = 3 mm) intracranial aneurysms
- PMID: 19131407
- PMCID: PMC7051764
- DOI: 10.3174/ajnr.A1429
Clinical and angiographic results of coiling of 196 very small (< or = 3 mm) intracranial aneurysms
Abstract
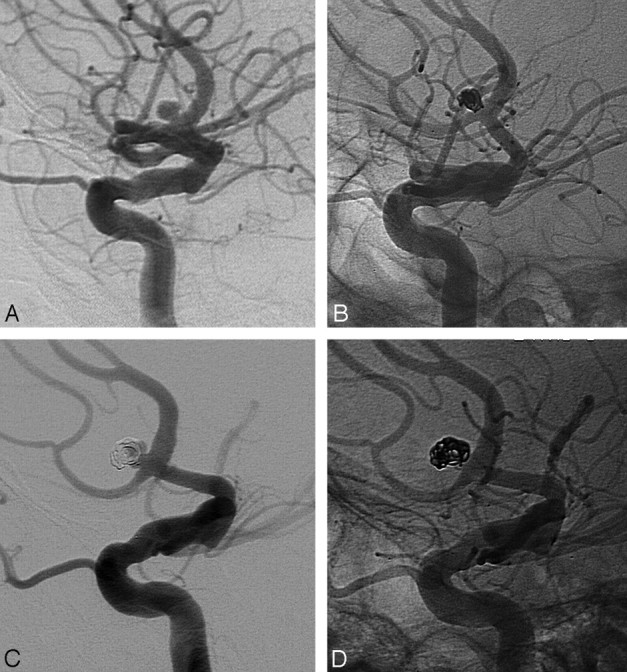
Background and purpose: Coiling of very small (< or = 3 mm) aneurysms is considered controversial because of technical difficulties and a higher rate of procedural aneurysm ruptures. In this study, we report clinical and angiographic results of coiling of aneurysms 3 mm or smaller in comparison with larger aneurysms in a large, single-center cohort of patients.
Materials and methods: Between 1995 and July 2008, a total of 1295 aneurysms were selectively occluded with coils. Of 1295 aneurysms, 196 (15.1%) in 187 patients were very small. Of 196 aneurysms, 149 (76%) had ruptured and 47 (24%) had not ruptured. There were 51 males (27%) and 136 females (73%). Mean age was 54.7 years (age range, 11-78 years).
Results: Procedural morbidity rate was 2.1% and mortality rate, 1.1%. Procedural rupture occurred in 15 of 196 aneurysms (7.7%). In 13 of 15 procedural ruptures, this had no adverse effect on outcome. Early recurrent hemorrhage of the coiled aneurysm occurred in 2 patients (1.1%). Compared with larger aneurysms, in very small aneurysms more often a procedural rupture occurred (7.7% versus 3.6%; P = .018). Procedural morbidity rate was lower (3.2% versus 5.5%), but this was not significant (P = .26). Retreatment rate consisted predominantly of clipping soon after incomplete coiling and was lower than in larger aneurysms (5.1% versus 10.0%; P = .041). Other characteristics were not significantly different.
Conclusions: Coiling of very small aneurysms was technically feasible, with good results. Although procedural aneurysm rupture was significantly more frequent in very small aneurysms, this did not lead to increased overall morbidity and mortality rates. Retreatment rate was lower than for larger aneurysms.
Figures
Comment in
-
Intraprocedural rupture of aneurysms: not necessarily a small problem.AJNR Am J Neuroradiol. 2009 Oct;30(9):E131; author reply E132. doi: 10.3174/ajnr.A1759. Epub 2009 Jul 23. AJNR Am J Neuroradiol. 2009. PMID: 19628628 Free PMC article. No abstract available.
References
-
- Molyneux A, Kerr R, Stratton I, et al. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group: International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised trial. Lancet 2002;360:1267–74 - PubMed
-
- Suzuki S, Kurata A, Ohmomo T, et al. Endovascular surgery for very small ruptured intracranial aneurysms. Technical note. J Neurosurg 2006;105:777–80 - PubMed
-
- Lim YC, Kim BM, Shin YS, et al. Structural limitations of currently available microcatheters and coils for endovascular coiling of very small aneurysms Neuroradiology 2008;50:423–27 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical