

Acute rejection and humoral sensitization in lung transplant recipients
- PMID: 19131531
- PMCID: PMC2626504
- DOI: 10.1513/pats.200808-080GO
Acute rejection and humoral sensitization in lung transplant recipients
Abstract
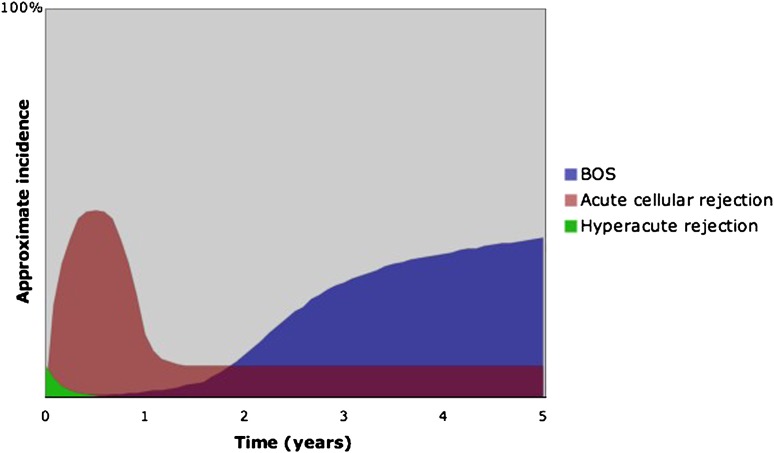
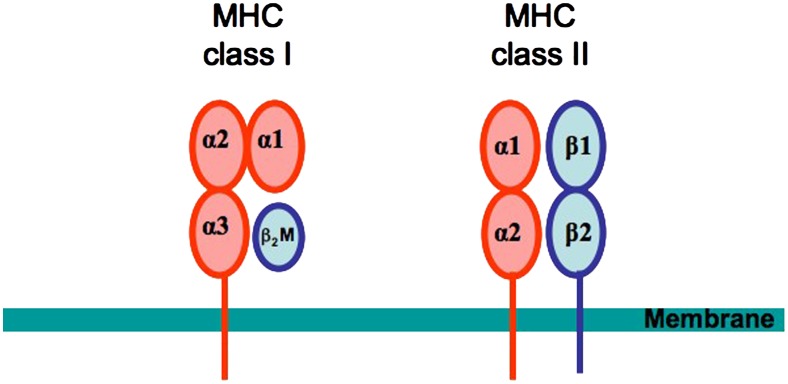
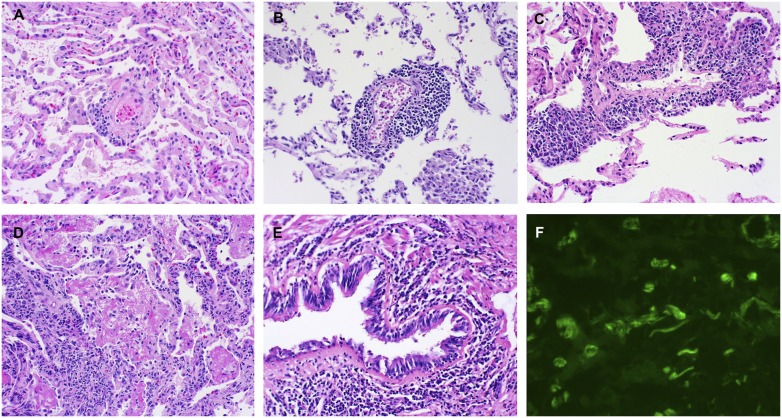
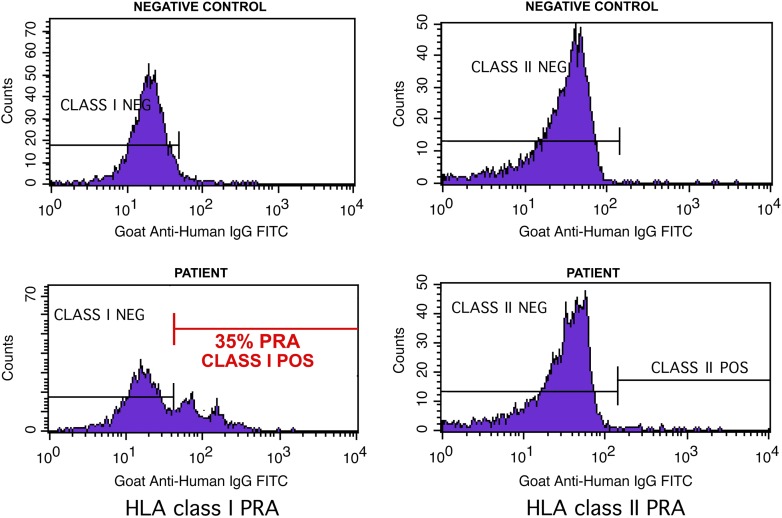
Despite the recent introduction of many improved immunosuppressive agents for use in transplantation, acute rejection affects up to 55% of lung transplant recipients within the first year after transplant. Acute lung allograft rejection is defined as perivascular or peribronchiolar mononuclear inflammation. Although histopathologic signs of rejection often resolve with treatment, the frequency and severity of acute rejections represent the most important risk factor for the subsequent development of bronchiolitis obliterans syndrome (BOS), a condition of progressive airflow obstruction that limits survival to only 50% at 5 years after lung transplantation. Recent evidence demonstrates that peribronchiolar mononuclear inflammation (also known as lymphocytic bronchiolitis) or even a single episode of minimal perivascular inflammation significantly increase the risk for BOS. We comprehensively review the clinical presentation, diagnosis, histopathologic features, and mechanisms of acute cellular lung rejection. In addition, we consider emerging evidence that humoral rejection occurs in lung transplantation, characterized by local complement activation or the presence of antibody to donor human leukocyte antigens (HLA). We discuss in detail methods for HLA antibody detection as well as the clinical relevance, the mechanisms, and the pathologic hallmarks of humoral injury. Treatment options for cellular rejection include high-dose methylprednisolone, antithymocyte globulin, or alemtuzumab. Treatment options for humoral rejection include intravenous immunoglobulin, plasmapheresis, or rituximab. A greater mechanistic understanding of cellular and humoral forms of rejection and their role in the pathogenesis of BOS is critical in developing therapies that extend long-term survival after lung transplantation.
Figures
References
-
- Trulock EP, Christie JD, Edwards LB, Boucek MM, Aurora P, Taylor DO, Dobbels F, Rahmel AO, Keck BM, Hertz MI. Registry of the international society for heart and lung transplantation: twenty-fourth official adult lung and heart-lung transplantation report-2007. J Heart Lung Transplant 2007;26:782–795. - PubMed
-
- Sharples LD, McNeil K, Stewart S, Wallwork J. Risk factors for bronchiolitis obliterans: asystematic review of recent publications. J Heart Lung Transplant 2002;21:271–281. - PubMed
-
- Snyder LD, Palmer SM. Immune mechanisms of lung allograft rejection. Semin Respir Crit Care Med 2006;27:534–543. - PubMed
-
- Lau CL, Palmer SM, D'Amico TA, Tapson VF, Davis RD. Lung transplantation at Duke University Medical Center. Clin Transpl 1998;327–340. - PubMed
-
- Sarahrudi K, Carretta A, Wisser W, Senbaklavaci O, Ploner M, Neuhauser P, Dobrovits M, Miwai Marta G, Papp A, Klepetko W. The value of switching from cyclosporine to tacrolimus in the treatment of refractory acute rejection and obliterative bronchiolitis after lung transplantation. Transpl Int 2002;15:24–28. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials