

Acute mixed lineage leukemia in children: the experience of St Jude Children's Research Hospital
- PMID: 19131545
- PMCID: PMC2686179
- DOI: 10.1182/blood-2008-10-187351
Acute mixed lineage leukemia in children: the experience of St Jude Children's Research Hospital
Abstract
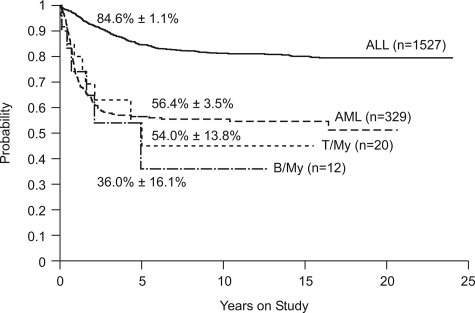
To characterize the biology and optimal therapy of acute mixed-lineage leukemia in children, we reviewed the pathologic and clinical features, including response to therapy, of 35 patients with mixed-lineage leukemia. The majority of cases (91%) had blasts cells that simultaneously expressed either T-lineage plus myeloid markers (T/myeloid, n = 20) or B-lineage plus myeloid markers (B/myeloid, n = 12). Overall survival rates for the B/myeloid and T/myeloid subgroups were not significantly different from each other or from the rate for acute myeloid leukemia (AML) but were inferior to the outcome in children with acute lymphoblastic leukemia (ALL). Patients who failed to achieve complete remission with AML-directed therapy could often be induced with a regimen of prednisone, vincristine, and L-asparaginase. Analysis of gene-expression patterns identified a subset of biphenotypic leukemias that did not cluster with T-cell ALL, B-progenitor ALL, or AML. We propose that treatment for biphenotypic leukemia begin with one course of AML-type induction therapy, with a provision for a switch to lymphoid-type induction therapy with a glucocorticoid, vincristine, and L-asparaginase if the patient responds poorly. We also suggest that hematopoietic stem cell transplantation is often not required for cure of these patients.
Figures

Comment in
-
Apples and oranges: mixed lineage acute leukemia.Blood. 2009 May 21;113(21):5036. doi: 10.1182/blood-2009-02-203232. Blood. 2009. PMID: 19470432 No abstract available.
References
-
- Mirro J, Zipf TF, Pui CH, et al. Acute mixed lineage leukemia: clinicopathologic correlations and prognostic significance. Blood. 1985;66:1115–1123. - PubMed
-
- Pui CH, Behm FG, Singh B, et al. Myeloid-associated antigen expression lacks prognostic value in childhood acute lymphoblastic leukemia treated with intensive multiagent chemotherapy. Blood. 1990;75:198–202. - PubMed
-
- Pui CH, Raimondi SC, Head DR, et al. Characterization of childhood acute leukemia with multiple myeloid and lymphoid markers at diagnosis and at relapse. Blood. 1991;78:1327–1337. - PubMed
-
- Wiersma SR, Ortega J, Sobel E, Weinberg KI. Clinical importance of myeloid-antigen expression in acute lymphoblastic leukemia of childhood. N Engl J Med. 1991;324:800–808. - PubMed
-
- Uckun FM, Sather HN, Gaynon PS, et al. Clinical features and treatment outcome of children with myeloid antigen positive acute lymphoblastic leukemia: a report from the Children's Cancer Group. Blood. 1997;90:28–35. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
