

Increasing burden of melanoma in the United States
- PMID: 19131946
- PMCID: PMC2866180
- DOI: 10.1038/jid.2008.423
Increasing burden of melanoma in the United States
Abstract
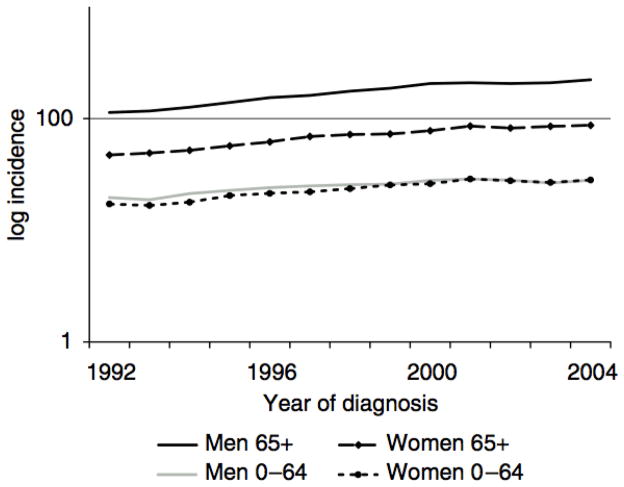
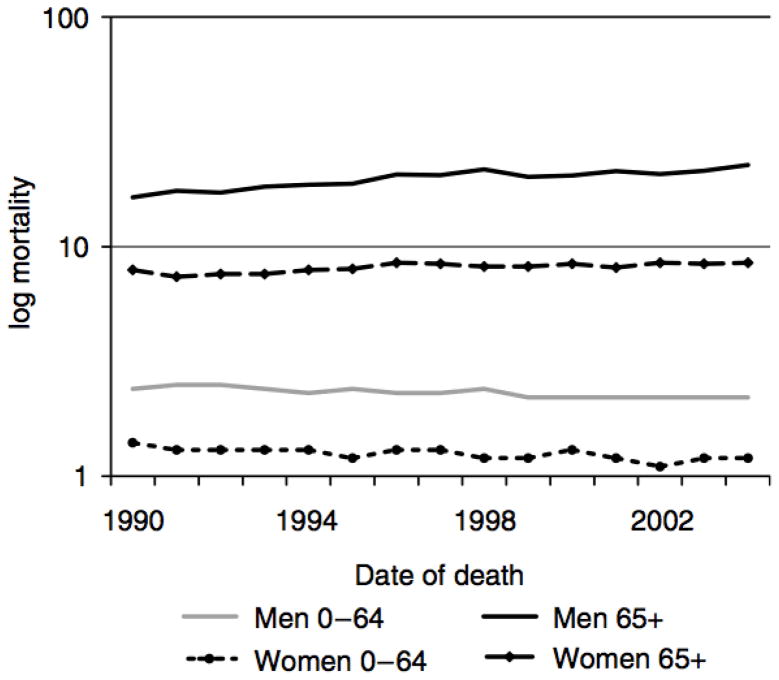
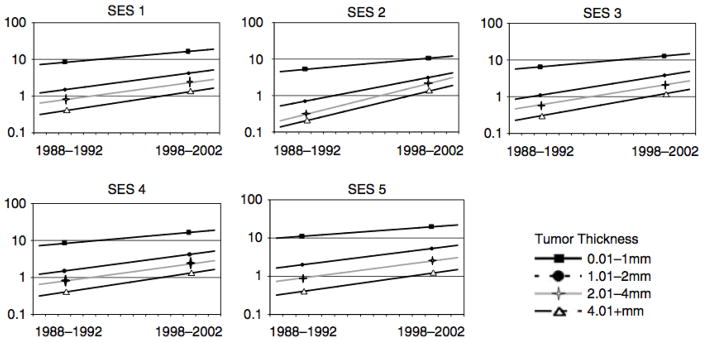
It is controversial whether worldwide increases in melanoma incidence represent a true epidemic. Dramatic increases in incidence in the setting of relatively stable mortality trends have also been attributed to expanded skin screening and detection of biologically indolent tumors with low metastatic potential. To better understand how melanoma incidence trends varied by severity at diagnosis and factors relevant to screening access, we assessed recent United States incidence and mortality trends by histologic type, tumor thickness, and area-level socioeconomic status (SES). We obtained population-based data regarding diagnoses of invasive melanoma among non-Hispanic whites from nearly 291 million person-years of observation by the Surveillance Epidemiology and End Results (SEER) program (1992-2004). Age-adjusted incidence and mortality rates were calculated for SEER and a subset (California) for which small-area SES measure was available. Overall, melanoma incidence increased at 3.1% (P<0.001) per year. Statistically significant rises occurred for tumors of all histologic subtypes and thicknesses, including those >4 mm. Melanoma incidence rates doubled in all SES groups over a 10-year period whereas melanoma mortality rates did not increase significantly. We conclude that screening-associated diagnosis of thinner melanomas cannot explain the increasing rates of thicker melanomas among low SES populations with poorer access to screening.
Conflict of interest statement
The authors state no conflict of interest.
Figures
Comment in
-
Melanoma is up: are we up to this challenge?J Invest Dermatol. 2009 Jul;129(7):1604-6. doi: 10.1038/jid.2009.115. J Invest Dermatol. 2009. PMID: 19521406
References
-
- Kleinbaum DG. Applied regression analysis and other multivariable methods. 2. Boston: PSW Kent; 1988.
-
- SEER*Stat software, version 6.1.4. Bethesda MD: Surveillance Research Program, National Cancer institute; 2005.
-
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Mortality - All COD, Public-Use With State, Total U.S. (1990–2004), National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2007. Underlying mortality data provided by NCHS. ( www.seer.cancer.gov) ( www.cdc.gov/nchs)
-
- Balch CM, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, et al. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J Clin Oncol. 2001a;19:3635–3648. - PubMed
-
- Balch CM, Soong SJ, Gershenwald JE, Thompson JF, Reintgen DS, Cascinelli N, et al. Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol. 2001b;19:3622–3634. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
