

Modeling the invasion of community-acquired methicillin-resistant Staphylococcus aureus into hospitals
- PMID: 19137654
- PMCID: PMC2666259
- DOI: 10.1086/595844
Modeling the invasion of community-acquired methicillin-resistant Staphylococcus aureus into hospitals
Abstract
Background: Methicillin-resistant Staphylococcus aureus (MRSA) has traditionally been associated with infections in hospitals. Recently, a new strain of MRSA has emerged and rapidly spread in the community, causing serious infections among young, healthy individuals. Preliminary reports imply that a particular clone (USA300) of a community-acquired MRSA (CA-MRSA) strain is infiltrating hospitals and replacing the traditional hospital-acquired MRSA strains. If true, this event would have serious consequences, because CA-MRSA infections in hospitals would occur among a more debilitated, older patient population.
Methods: A deterministic mathematical model was developed to characterize the factors contributing to the replacement of hospital-acquired MRSA with CA-MRSA and to quantify the effectiveness of interventions aimed at limiting the spread of CA-MRSA in health care settings.
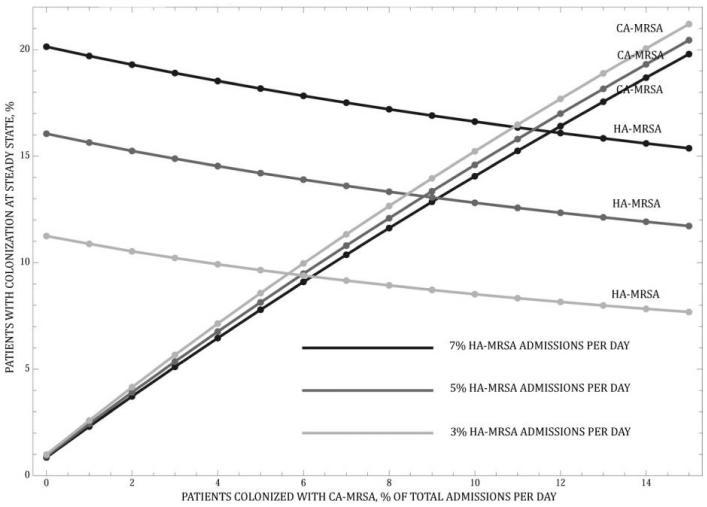
Results: The model strongly suggests that CA-MRSA will become the dominant MRSA strain in hospitals and health care facilities. This reversal of dominant strain will occur as a result of the documented expanding community reservoir and increasing influx into the hospital of individuals who harbor CA-MRSA. Competitive exclusion of hospital-acquired MRSA by CA-MRSA will occur, with increased severity of CA-MRSA infections resulting in longer hospitalizations and a larger in-hospital reservoir of CA-MRSA.
Conclusions: Improving compliance with hand hygiene and screening for and decolonization of CA-MRSA carriers are effective strategies. However, hand hygiene has the greatest return of benefits and, if compliance is optimized, other strategies may have minimal added benefit.
Figures






References
-
- Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. 2007;298:1763–71. - PubMed
-
- Bancroft EA. Antimicrobial resistance, it’s not just for hospitals. JAMA. 2007;298:1803–4. - PubMed
-
- Herold BC, Immergluck LC, Maranan LC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279:593–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
