

Recommendations for implementing stereotactic radiotherapy in peripheral stage IA non-small cell lung cancer: report from the Quality Assurance Working Party of the randomised phase III ROSEL study
- PMID: 19138400
- PMCID: PMC2631491
- DOI: 10.1186/1748-717X-4-1
Recommendations for implementing stereotactic radiotherapy in peripheral stage IA non-small cell lung cancer: report from the Quality Assurance Working Party of the randomised phase III ROSEL study
Abstract
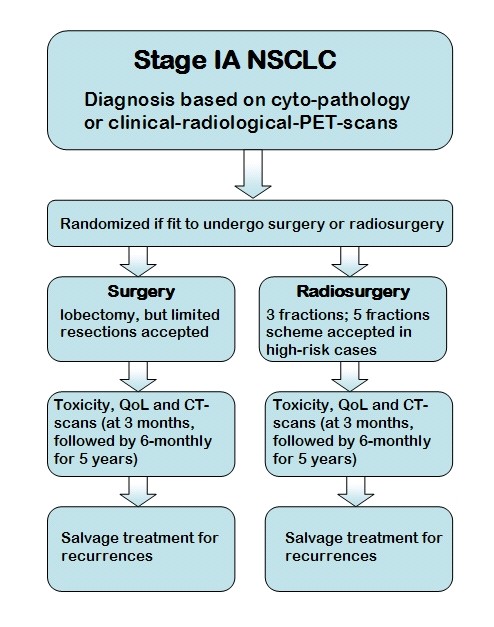
Background: A phase III multi-centre randomised trial (ROSEL) has been initiated to establish the role of stereotactic radiotherapy in patients with operable stage IA lung cancer. Due to rapid changes in radiotherapy technology and evolving techniques for image-guided delivery, guidelines had to be developed in order to ensure uniformity in implementation of stereotactic radiotherapy in this multi-centre study.
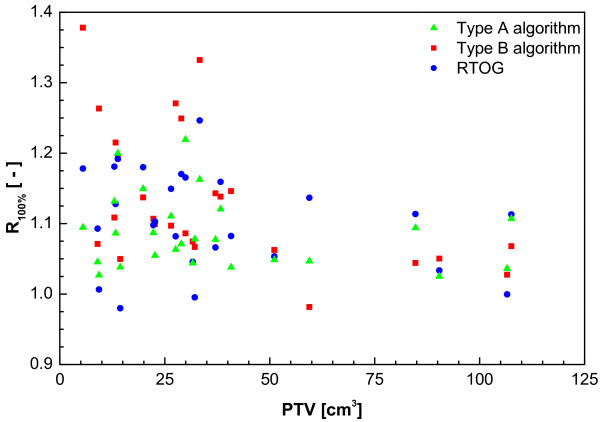
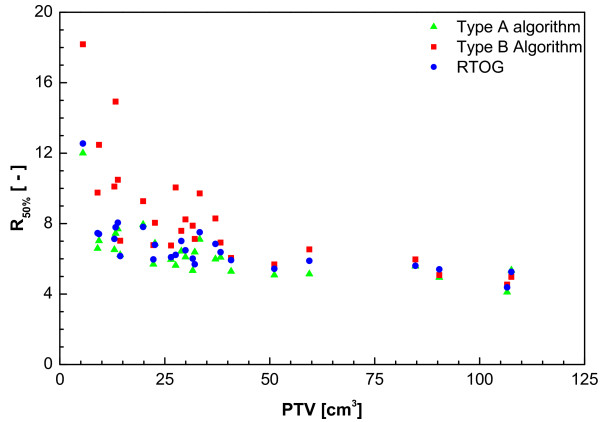
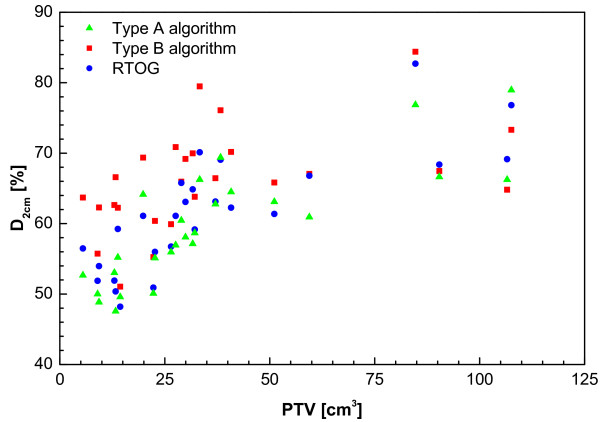
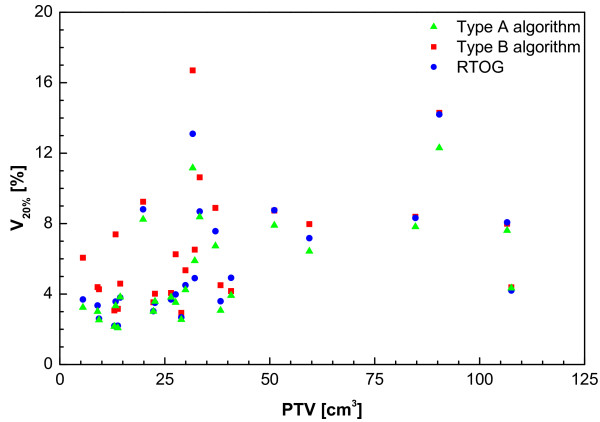
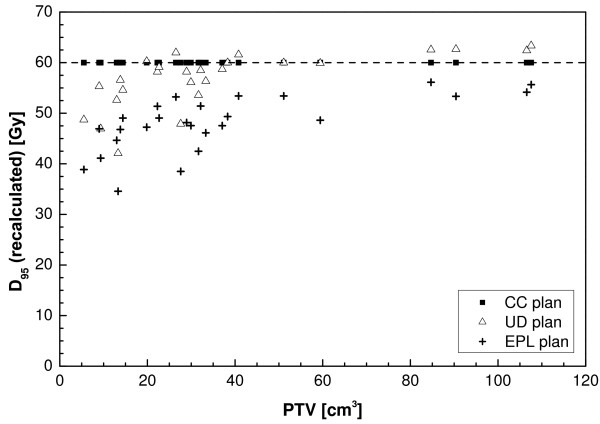
Methods/design: A Quality Assurance Working Party was formed by radiation oncologists and clinical physicists from both academic as well as non-academic hospitals that had already implemented stereotactic radiotherapy for lung cancer. A literature survey was conducted and consensus meetings were held in which both the knowledge from the literature and clinical experience were pooled. In addition, a planning study was performed in 26 stage I patients, of which 22 were stage 1A, in order to develop and evaluate the planning guidelines. Plans were optimised according to parameters adopted from RTOG trials using both an algorithm with a simple homogeneity correction (Type A) and a more advanced algorithm (Type B). Dose conformity requirements were then formulated based on these results.
Conclusion: Based on current literature and expert experience, guidelines were formulated for this phase III study of stereotactic radiotherapy versus surgery. These guidelines can serve to facilitate the design of future multi-centre clinical trials of stereotactic radiotherapy in other patient groups and aid a more uniform implementation of this technique outside clinical trials.
Figures
References
-
- Nagata Y, Takayama K, Matsuo Y, Norihisa Y, Mizowaki T, Sakamoto T, Sakamoto M, Mitsumori M, Shibuya K, Araki N, Yano S, Hiraoka M. Clinical outcomes of a phase I/II study of 48 Gy of stereotactic body radiotherapy in 4 fractions for primary lung cancer using a stereotactic body frame. Int J Radiat Oncol Biol Phys. 2005;63:1427–1431. doi: 10.1016/j.ijrobp.2005.05.034. - DOI - PubMed
-
- Onishi H, Shirato H, Nagata Y, Hiraoka M, Fujino M, Gomi K, Niibe Y, Karasawa K, Hayakawa K, Takai Y, Kimura T, Takeda A, Ouchi A, Hareyama M, Kokubo M, Hara R, Itami J, Yamada K, Araki T. Hypofractionated stereotactic radiotherapy (HypoFXSRT) for stage I non-small cell lung cancer: updated results of 257 patients in a Japanese multi-institutional study. J Thorac Oncol. 2007;2:S94–100. doi: 10.1097/JTO.0b013e318074de34. - DOI - PubMed
-
- McGarry RC, Papiez L, Williams M, Whitford T, Timmerman RD. Stereotactic body radiation therapy of early-stage non-small-cell lung carcinoma: phase I study. Int J Radiat Oncol Biol Phys. 2006;63:1010–1015. - PubMed
-
- Lagerwaard FJ, Haasbeek CJA, Smit EF, Slotman BJ, Senan S. Outcome After Stereotactic Radiotherapy in 'High-Risk' Patients With Stage I Non-small Cell Lung Cancer (NSCLC) Int J Radiat Oncol Biol Phys. 2007;69:S87–S88.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
