

A prediction model for lung cancer diagnosis that integrates genomic and clinical features
- PMID: 19138936
- PMCID: PMC4167688
- DOI: 10.1158/1940-6207.CAPR-08-0011
A prediction model for lung cancer diagnosis that integrates genomic and clinical features
Abstract
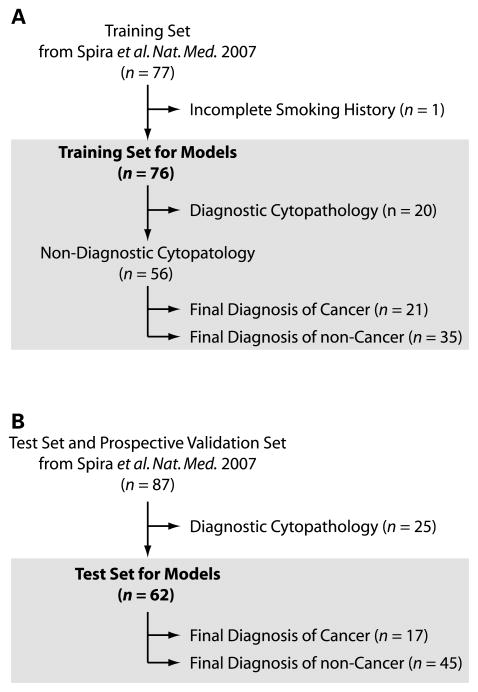
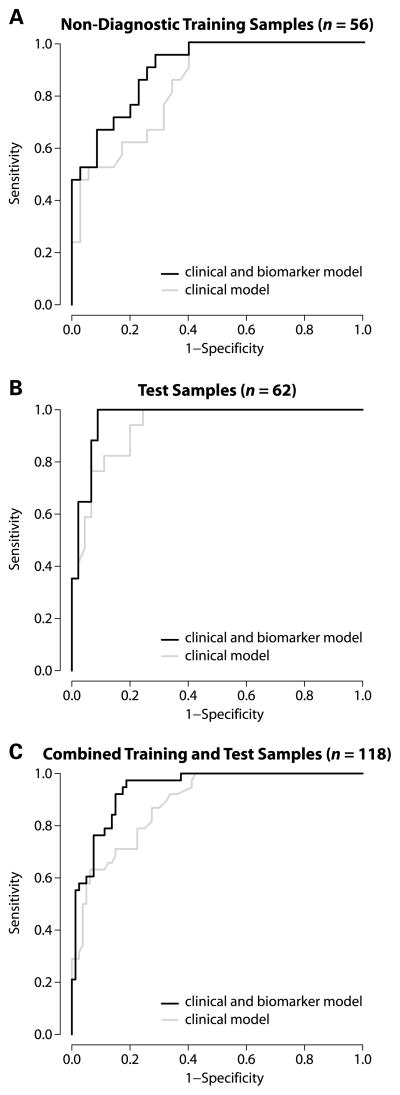
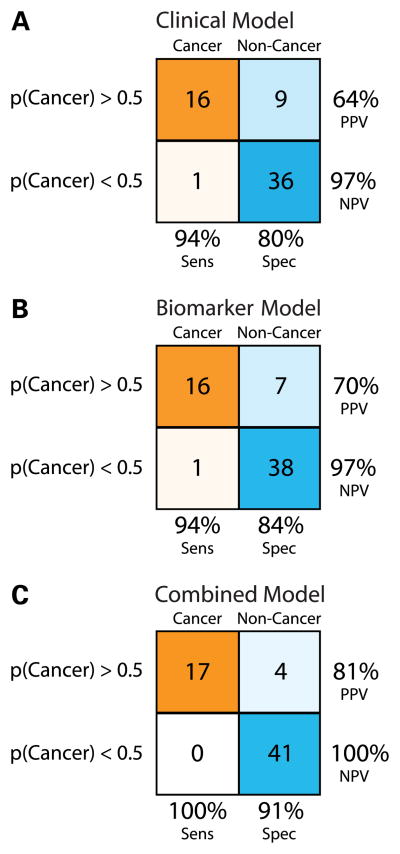
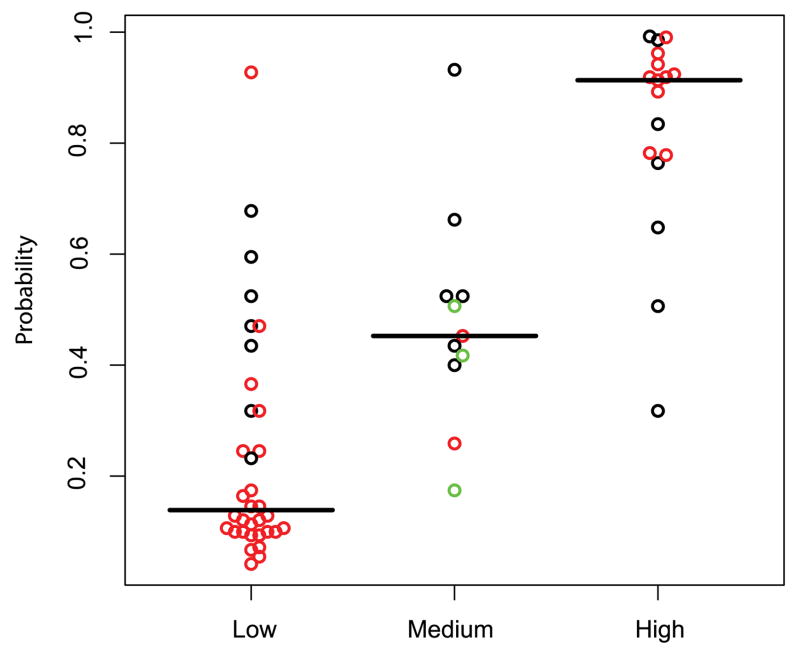
Lung cancer is the leading cause of cancer death due, in part, to lack of early diagnostic tools. Bronchoscopy represents a relatively noninvasive initial diagnostic test in smokers with suspect disease, but it has low sensitivity. We have reported a gene expression profile in cytologically normal large airway epithelium obtained via bronchoscopic brushings, which is a sensitive and specific biomarker for lung cancer. Here, we evaluate the independence of the biomarker from other clinical risk factors and determine the performance of a clinicogenomic model that combines clinical factors and gene expression. Training (n = 76) and test (n = 62) sets consisted of smokers undergoing bronchoscopy for suspicion of lung cancer at five medical centers. Logistic regression models describing the likelihood of having lung cancer using the biomarker, clinical factors, and these data combined were tested using the independent set of patients with nondiagnostic bronchoscopies. The model predictions were also compared with physicians' clinical assessment. The gene expression biomarker is associated with cancer status in the combined clinicogenomic model (P < 0.005). There is a significant difference in performance of the clinicogenomic relative to the clinical model (P < 0.05). In the test set, the clinicogenomic model increases sensitivity and negative predictive value to 100% and results in higher specificity (91%) and positive predictive value (81%) compared with other models. The clinicogenomic model has high accuracy where physician assessment is most uncertain. The airway gene expression biomarker provides information about the likelihood of lung cancer not captured by clinical factors, and the clinicogenomic model has the highest prediction accuracy. These findings suggest that use of the clinicogenomic model may expedite more invasive testing and definitive therapy for smokers with lung cancer and reduce invasive diagnostic procedures for individuals without lung cancer.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Shields PG. Molecular epidemiology of lung cancer. Ann Oncol. 1999;10 (Suppl 5):S7–11. - PubMed
-
- Hoffman PC, Mauer AM, Vokes EE. Lung cancer. Lancet. 2000;355:479–85. - PubMed
-
- Postmus PE. Bronchoscopy for lung cancer. Chest. 2005;128:16–8. - PubMed
-
- Mazzone P, Jain P, Arroliga AC, Matthay RA. Bronchoscopy and needle biopsy techniques for diagnosis and staging of lung cancer. Clin Chest Med. 2002;23:137–58. ix. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
