

Joint effects of sodium and potassium intake on subsequent cardiovascular disease: the Trials of Hypertension Prevention follow-up study
- PMID: 19139321
- PMCID: PMC2629129
- DOI: 10.1001/archinternmed.2008.523
Joint effects of sodium and potassium intake on subsequent cardiovascular disease: the Trials of Hypertension Prevention follow-up study
Abstract
Background: Previous studies of dose-response effects of usual sodium and potassium intake on subsequent cardiovascular disease (CVD) have largely relied on suboptimal measures of intake.
Methods: Two trials of sodium reduction and other interventions collected 24-hour urinary excretions intermittently during 18 months from September 17, 1987, to January 12, 1990 (Trials of Hypertension Prevention [TOHP] I), and during 36 months from December 18, 1990, to April 7, 1995 (TOHP II), among adults with prehypertension aged 30 to 54 years. Among adults not assigned to an active sodium reduction intervention, we assessed the relationship of a mean of 3 to 7 twenty-four-hour urinary excretions of sodium and potassium and their ratio with subsequent CVD (stroke, myocardial infarction, coronary revascularization, or CVD mortality) through 10 to 15 years of posttrial follow-up.
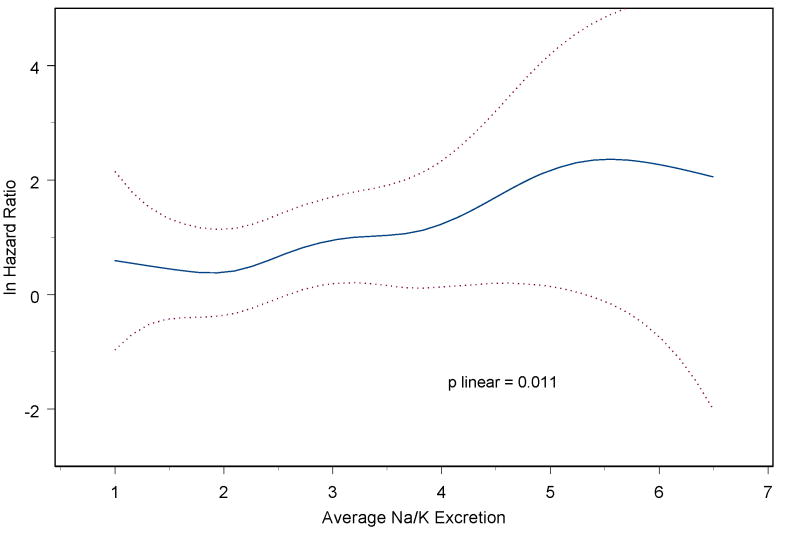
Results: Among 2974 participants, follow-up information was obtained on 2275 participants (76.5%), with 193 CVD events. After adjustment for baseline variables and lifestyle changes, there was a nonsignificant trend in CVD risk across sex-specific quartiles of urinary sodium excretion (rate ratio [RR] from lowest to highest, 1.00, 0.99, 1.16, and 1.20; P = .38 for trend) and potassium excretion (RR, 1.00, 0.94, 0.91, and 0.64; P = .08 for trend) but a significant trend across quartiles of the sodium to potassium excretion ratio (RR, 1.00, 0.84, 1.18, and 1.50; P = .04 for trend). In models containing both measures simultaneously, linear effects were as follows: RR, 1.42; 95% confidence interval (CI), 0.99 to 2.04 per 100 mmol/24 h of urinary sodium excretion (P = .05); and 0.67; 0.41 to 1.10 per 50 mmol/24 h of urinary potassium excretion (P = .12). A model containing the sodium to potassium excretion ratio (RR, 1.24; 95% CI, 1.05-1.46; P = .01) had the lowest Bayes information criterion (best fit).
Conclusion: A higher sodium to potassium excretion ratio is associated with increased risk of subsequent CVD, with an effect stronger than that of sodium or potassium alone.
Figures
Comment in
-
Shared primacy of sodium and potassium on cardiovascular risk.Am J Kidney Dis. 2009 Oct;54(4):598-601. doi: 10.1053/j.ajkd.2009.05.008. Epub 2009 Jul 4. Am J Kidney Dis. 2009. PMID: 19577349 No abstract available.
References
-
- The Trials of Hypertension Prevention Collaborative Research Group. Effects of weight loss and sodium reduction intervention on blood pressure and hypertension incidence in overweight people with high- normal blood pressure. The Trials of Hypertension Prevention, Phase II. The Trials of Hypertension Prevention Collaborative Research Group. Arch Intern Med. 1997;157:657–667. - PubMed
-
- Whelton PK, He J, Cutler JA, et al. The effects of oral potassium on blood pressure: a quantitative overview of randomized, controlled clinical trials. J Amer Med Assoc. 1997;277:1624–1632. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL37849/HL/NHLBI NIH HHS/United States
- HL37853/HL/NHLBI NIH HHS/United States
- HL37907/HL/NHLBI NIH HHS/United States
- HL37899/HL/NHLBI NIH HHS/United States
- HL37852/HL/NHLBI NIH HHS/United States
- HL37872/HL/NHLBI NIH HHS/United States
- HL37884/HL/NHLBI NIH HHS/United States
- HL57915/HL/NHLBI NIH HHS/United States
- HL37924/HL/NHLBI NIH HHS/United States
- HL37854/HL/NHLBI NIH HHS/United States
- HL37904/HL/NHLBI NIH HHS/United States
- HL37906/HL/NHLBI NIH HHS/United States
- R01 HL057915/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
