

Continuity of care and intensive care unit use at the end of life
- PMID: 19139328
- PMCID: PMC2745737
- DOI: 10.1001/archinternmed.2008.514
Continuity of care and intensive care unit use at the end of life
Abstract
Background: There is increasing concern about discontinuity of care across transitions (eg, from home to the hospital) and how it might affect appropriate medical management.
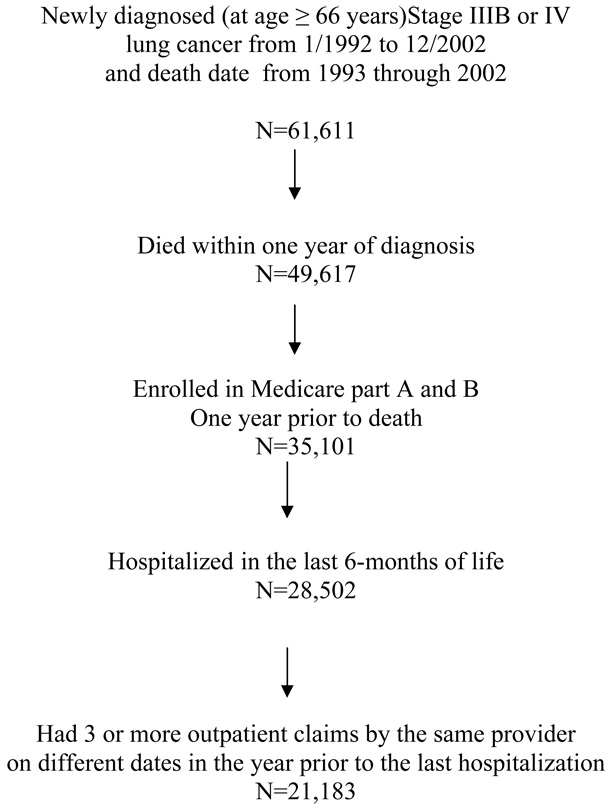
Methods: We examined changes over time in outpatient-to-inpatient continuity of care in individuals hospitalized with advanced lung cancer and its relationship to end-of-life intensive care unit (ICU) use via retrospective analysis of the linked Surveillance, Epidemiology, and End Results-Medicare database. Patients were 21 183 Medicare beneficiaries 66 years or older and diagnosed as having stage IIIB or IV lung cancer between January 1, 1992, and December 31, 2002, who died within a year of diagnosis. Outpatient-to-inpatient continuity of care was defined as an inpatient visit by the patient's usual care provider during the last hospitalization. The primary outcome measure was ICU use during the last hospitalization.
Results: Outpatient-to-inpatient continuity decreased from 60.1% in 1992 to 51.5% in 2002 (P < .001). Factors associated with decreased continuity included male sex, black race, low socioeconomic status, being unmarried, treatment by a hospitalist, and treatment in a teaching hospital. Use of the ICU increased by 5.8% per year from 1993 to 2002. After adjustment for patient characteristics, patients with outpatient-to-inpatient continuity of care had a 25.1% reduced odds of entering the ICU during their terminal hospitalization.
Conclusions: Outpatient-to-inpatient continuity of care declined during the 1990s and early 2000s. Patients with terminal lung cancer who experienced outpatient-to-inpatient continuity of care were less likely to spend time in the ICU before death.
Conflict of interest statement
Figures

References
-
- Institue of Medicine: National Academy of Sciences. 1st ed. Washington, DC: 1996. Committee on the future of primary care. Primary Care. America's health in new era.
-
- Gill JM, Mainous AG., III The role of provider continuity in preventing hospitalizations. Arch Fam Med. 1998 July;7(4):352–357. - PubMed
-
- Gill JM, Mainous AG, III, Nsereko M. The effect of continuity of care on emergency department use. Arch Fam Med. 2000 April;9(4):333–338. - PubMed
-
- Gill JM, Saldarriaga A, Mainous AG, III, Unger D. Does continuity between prenatal and well-child care improve childhood immunizations? Fam Med. 2002 April;34(4):274–280. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
