

Association between hyperglycemia and survival in patients with newly diagnosed glioblastoma
- PMID: 19139429
- PMCID: PMC2667812
- DOI: 10.1200/JCO.2008.19.1098
Association between hyperglycemia and survival in patients with newly diagnosed glioblastoma
Abstract
Purpose: Hyperglycemia has been associated with poor outcomes in many disease states. This retrospective study assessed the association between hyperglycemia and survival in patients with newly diagnosed glioblastoma multiforme (GBM). PATIENTS AND METHODS; Between 1999 and 2004, before the standard use of temozolomide, 191 patients were accrued onto New Approaches to Brain Tumor Therapy CNS Consortium trials with similar eligibility criteria. Time-weighted mean glucose and mean glucocorticoid dose were calculated for each patient using all values collected regularly in follow-up. The primary outcome was survival.
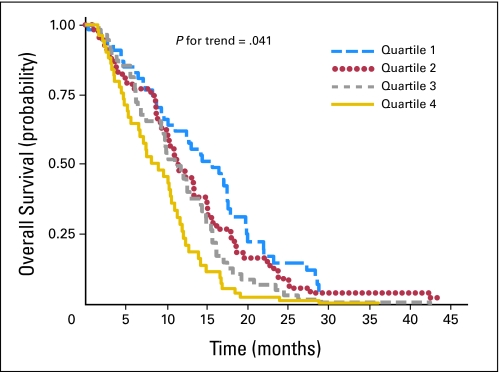
Results: Mean glucose levels ranged between 65 and 459 mg/dL. These were divided into quartiles: quartile one (< 94 mg/dL), quartile two (94 to 109 mg/dL), quartile three (110 to 137 mg/dL), and quartile four (> 137 mg/dL). Median survival times for patients in quartiles one, two, three, and four were 14.5, 11.6, 11.6, and 9.1 months, respectively. The association between higher mean glucose and shorter survival persisted after adjustment for mean daily glucocorticoid dose, age, and baseline Karnofsky performance score (KPS). Compared with patients in the lowest mean glucose quartile, those in quartile two (adjusted hazard ratio [HR], 1.29; 95% CI, 0.85 to 1.96), quartile three (adjusted HR, 1.35; 95% CI, 0.89 to 2.06), and quartile four (adjusted HR, 1.57; 95% CI, 1.02 to 2.40) were at progressively higher risk of dying (P = .041 for trend).
Conclusion: In these patients with newly diagnosed GBM and good baseline KPS, hyperglycemia was associated with shorter survival, after controlling for glucocorticoid dose and other confounders. The effect of intensive management of glucocorticoid-related hyperglycemia on survival deserves additional study in patients with GBM.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. - PubMed
-
- Malmberg K, Norhammar A, Wedel H, et al. Glycometabolic state at admission: Important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction—Long-term results from the diabetes and insulin-glucose infusion in acute myocardial infarction (DIGAMI) study. Circulation. 1999;99:2626–2632. - PubMed
-
- Weiser MA, Cabanillas ME, Konopleva M, et al. Relation between the duration of remission and hyperglycemia during induction chemotherapy for acute lymphocytic leukemia with a hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone/methotrexate-cytarabine regimen. Cancer. 2004;100:1179–1185. - PubMed
-
- Yancik R, Wesley MN, Ries LA, et al. Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA. 2001;285:885–892. - PubMed
-
- Polednak AP. Comorbid diabetes mellitus and risk of death after diagnosis of colorectal cancer: A population-based study. Cancer Detect Prev. 2006;30:466–472. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
