

Contrast-enhanced 3D ultrasound in the radiofrequency ablation of liver tumors
- PMID: 19140228
- PMCID: PMC2653325
- DOI: 10.3748/wjg.15.289
Contrast-enhanced 3D ultrasound in the radiofrequency ablation of liver tumors
Abstract
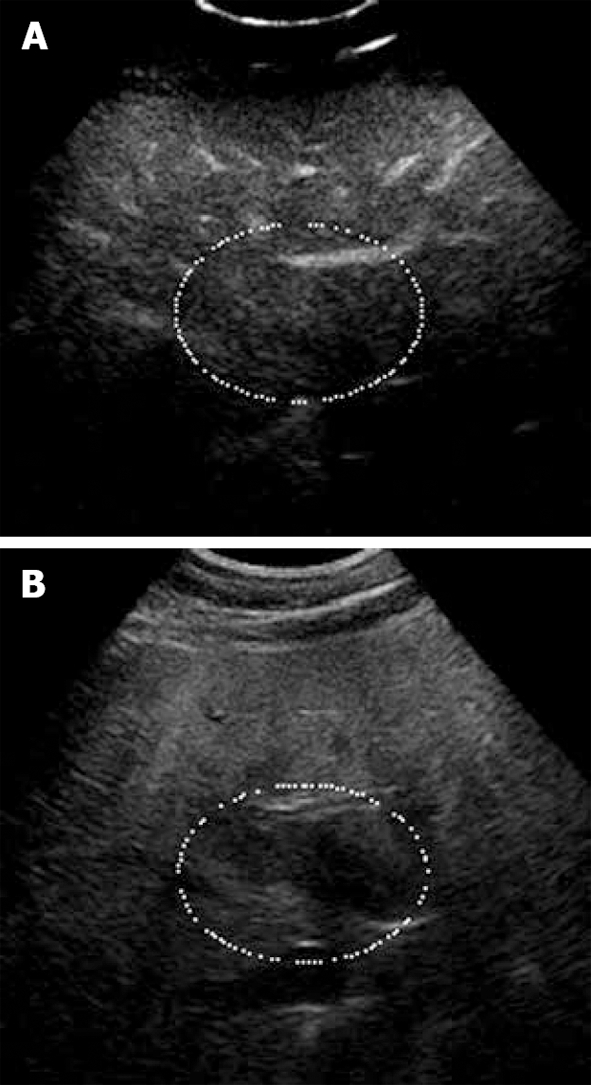
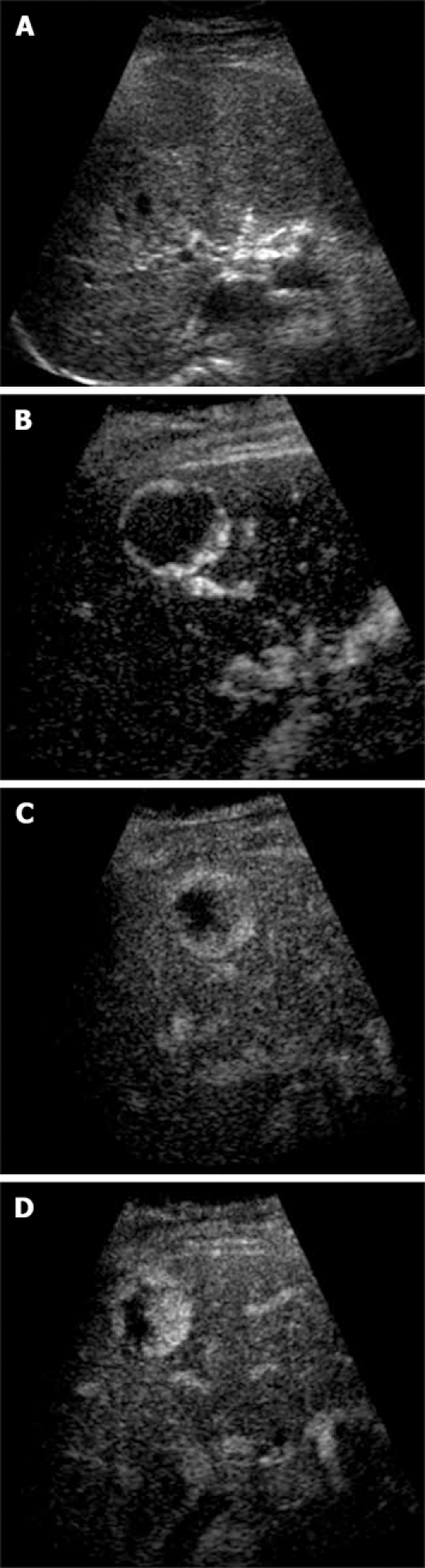
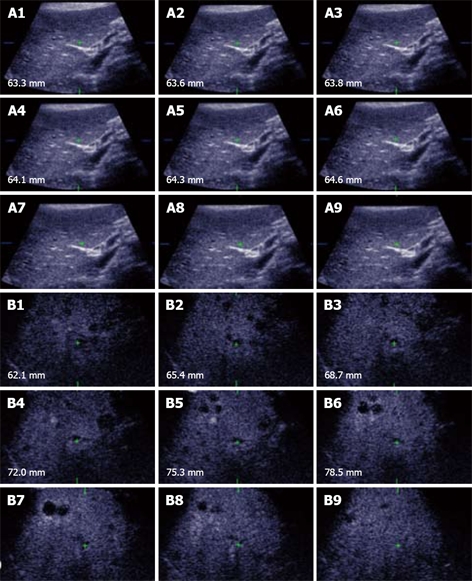
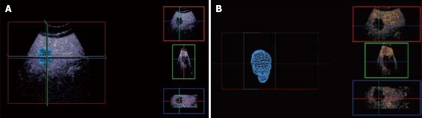
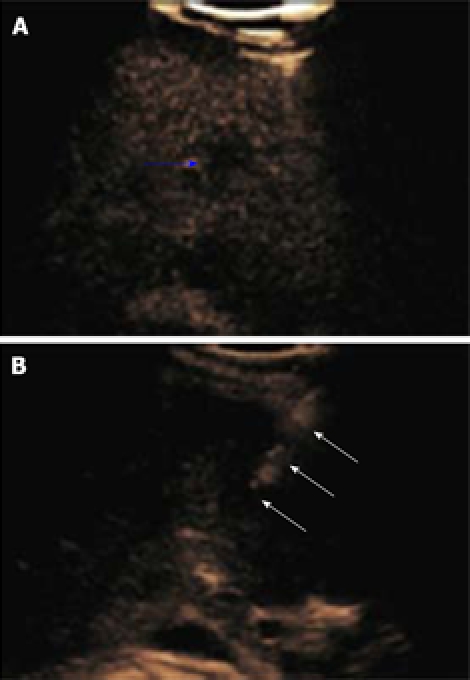
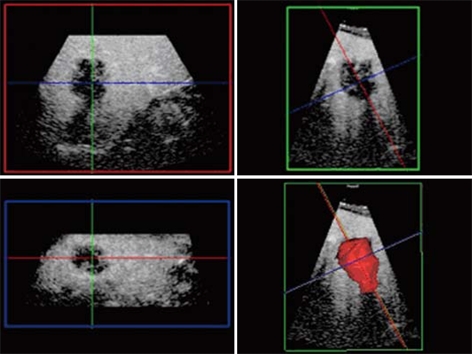
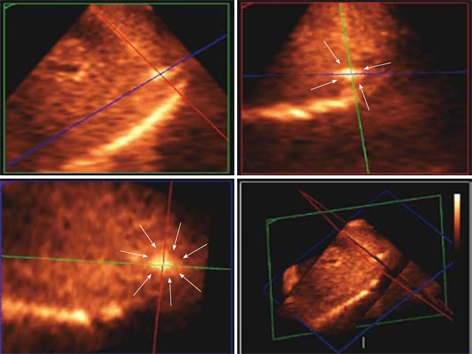
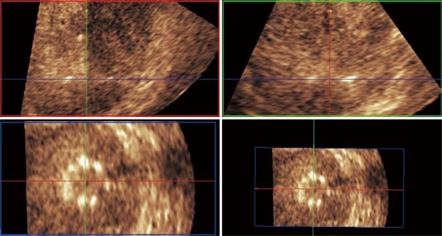
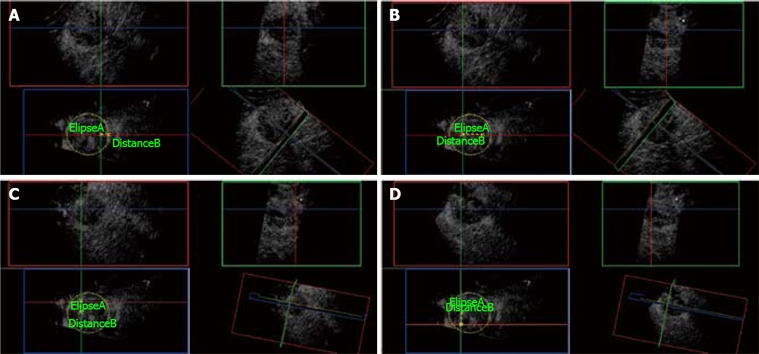
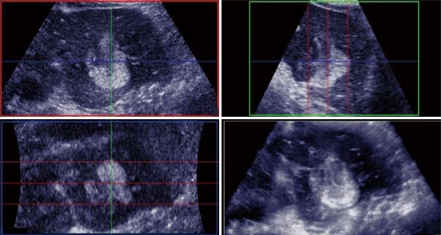
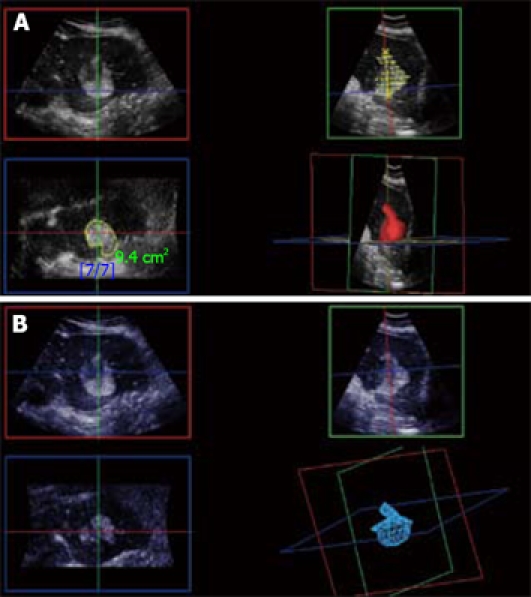
Liver metastases and hepatocellular carcinomas are two of the most common causes of cancer deaths in the world. Radiofrequency ablation (RFA) is a well recognized, effective and minimally invasive means of treating malignant hepatic tumors. This article describes the use of contrast-enhanced 3D ultrasound (CE-3DUS) in the staging, targeting and follow-up of patients with liver tumors undergoing RFA. In particular, its value in the management of large hepatic lesions will be illustrated. Current limitations of CE-3DUS and future developments in the technique will also be discussed. In summary, CE-3DUS is useful in the RFA of liver tumors with improved detection and display of occult lesions and recurrence, in the assessment of lesional geometry and orientation for a more accurate planning and guidance of multiple RFA needle electrodes in large tumors and in the evaluation of residual or recurrent disease within the immediate and/or subsequent follow-up periods.
Figures

References
-
- O'Brien MJ. Cancer of the colon and rectum: current concepts of aetiology and pathogenesis. Ir J Med Sci. 1988;157:5–15. - PubMed
-
- McArdle CS, Hole D, Hansell D, Blumgart LH, Wood CB. Prospective study of colorectal cancer in the west of Scotland: 10-year follow-up. Br J Surg. 1990;77:280–282. - PubMed
-
- Scheele J, Stang R, Altendorf-Hofmann A, Paul M. Resection of colorectal liver metastases. World J Surg. 1995;19:59–71. - PubMed
-
- Fong Y, Cohen AM, Fortner JG, Enker WE, Turnbull AD, Coit DG, Marrero AM, Prasad M, Blumgart LH, Brennan MF. Liver resection for colorectal metastases. J Clin Oncol. 1997;15:938–946. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
