

Meta-Analysis
doi: 10.1086/596482.
Better adherence with once-daily antiretroviral regimens: a meta-analysis
Affiliations
- PMID: 19140758
- PMCID: PMC2708315
- DOI: 10.1086/596482
Item in Clipboard
Meta-Analysis
Better adherence with once-daily antiretroviral regimens: a meta-analysis
Clin Infect Dis.
.
Abstract
Once-daily regimens of antiretroviral therapy are simpler than other regimens, but whether such regimens are associated with better adherence to treatment is controversial. We performed a meta-analysis of 11 randomized, controlled trials (total number of subjects, 3029), which revealed that the adherence rate was better with once-daily regimens (+2.9%; 95% confidence interval, 1.0%-4.8%; P < .003) than with twice-daily regimens. This modest effect was more pronounced at the time of treatment initiation and for regimens for which all medications were taken once per day.
Figures
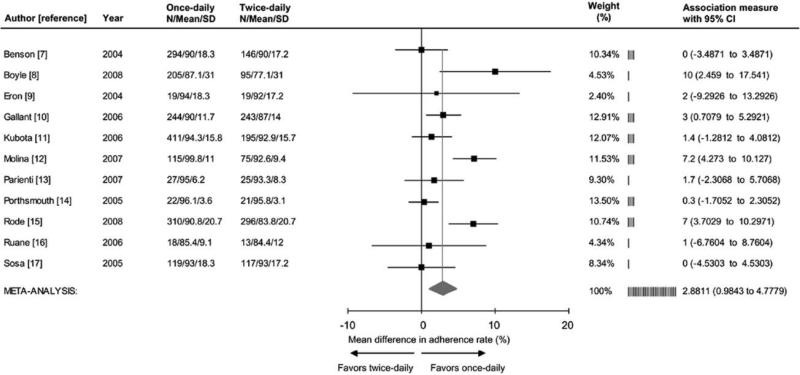
Forrest plot of the effect of once-daily versus twice-daily antiretroviral regimens on the rate of adherence. Adherence rate was defined as follows: (no. of taken doses/no. prescribed doses)×100. Cochrane Q test for heterogeneity: χ2=29.7; degrees of freedom, 10; P=<.001; I2=66.4%. Test for overall random effect: Z=2.98; P=<.003.
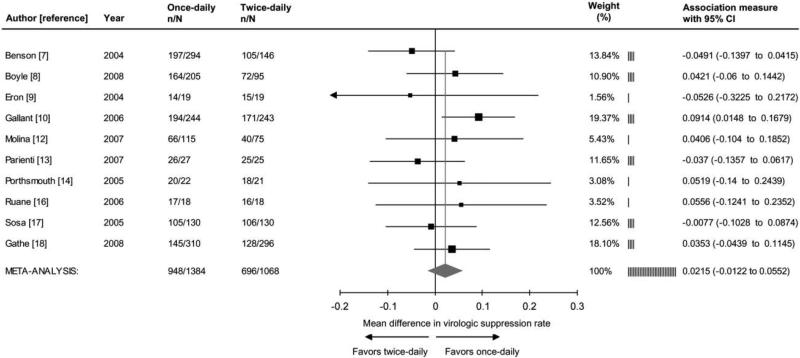
Forrest plot of the effect of once-daily versus twice-daily antiretroviral regimens on viral suppression. Viral suppression was defined as a plasma RNA HIV level <50 copies/mL in the intent-to-treat analysis, with missing equals failure. In the study by Gathe et al. [18], data represent week 12 results among subjects with Medication Event Monitoring System evaluation (Dr. Rode, personal communication, December 2008). Week 48 results are 77% and 76% for once-daily and twice-daily regimens, respectively. Cochrane Q test for heterogeneity: χ2=8.2; degrees of freedom, 9; P=.43; I2=0.0%. Test for overall random effect: Z=1.25; P=.21. n, No. of subjects with viral suppression; N, total sample size.
References
-
- Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133:21–30. - PubMed
-
- Bangsberg DR, Perry S, Charlebois ED, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15:1181–3. - PubMed
-
- Wood E, Hogg RS, Yip B, Harrigan PR, O'Shaughnessy MV, Montaner JS. Effect of medication adherence on survival of HIV-infected adults who start highly active antiretroviral therapy when the CD4+ cell count is 0.200 to 0.350 × 109 cells/L. Ann Intern Med. 2003;139:810–6. - PubMed
-
- Bartlett JA, Fath MJ, Demasi R, et al. An updated systematic overview of triple combination therapy in antiretroviral-naive HIV-infected adults. AIDS. 2006;20:2051–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
