

Inhaled drugs to reduce exacerbations in patients with chronic obstructive pulmonary disease: a network meta-analysis
- PMID: 19144173
- PMCID: PMC2636836
- DOI: 10.1186/1741-7015-7-2
Inhaled drugs to reduce exacerbations in patients with chronic obstructive pulmonary disease: a network meta-analysis
Abstract
Background: Most patients with chronic obstructive pulmonary disease (COPD) receive inhaled long-acting bronchodilators and inhaled corticosteroids. Conventional meta-analyses established that these drugs reduce COPD exacerbations when separately compared with placebo. However, there are relatively few head-to-head comparisons and conventional meta-analyses focus on single comparisons rather than on a simultaneous analysis of competing drug regimens that would allow rank ordering of their effectiveness. Therefore we assessed, using a network meta-analytic technique, the relative effectiveness of the common inhaled drug regimes used to reduce exacerbations in patients with COPD.
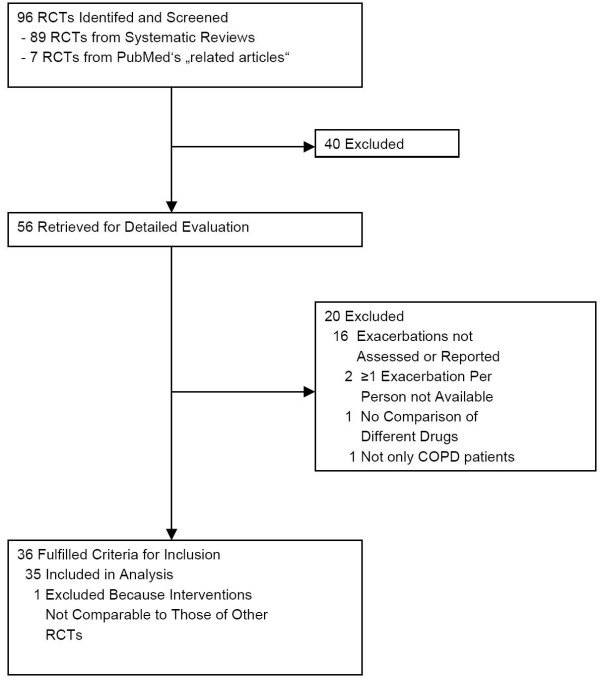
Methods: We conducted a systematic review and searched existing systematic reviews and electronic databases for randomized trials of >/= 4 weeks' duration that assessed the effectiveness of inhaled drug regimes on exacerbations in patients with stable COPD. We extracted participants and intervention characteristics from included trials and assessed their methodological quality. For each treatment group we registered the proportion of patients with >/= 1 exacerbation during follow-up. We used treatment-arm based logistic regression analysis to estimate the absolute and relative effects of inhaled drug treatments while preserving randomization within trials.
Results: We identified 35 trials enrolling 26,786 patients with COPD of whom 27% had >/= 1 exacerbation. All regimes reduced exacerbations statistically significantly compared with placebo (odds ratios ranging from 0.71 (95% confidence interval [CI] 0.64 to 0.80) for long-acting anticholinergics to 0.78 (95% CI 0.70 to 0.86) for inhaled corticosteroids). Compared with long-acting bronchodilators alone, combined treatment was not more effective (comparison with long-acting beta-agonists: odds ratio 0.93 [95% CI 0.84 to 1.04] and comparison with long-acting anticholinergics: odds ratio 1.02 [95% CI 0.90 to 1.16], respectively). If FEV1 was </= 40% predicted, long-acting anticholinergics, inhaled corticosteroids, and combination treatment reduced exacerbations significantly compared with long-acting beta-agonists alone, but not if FEV1 was > 40% predicted. This effect modification was significant for inhaled corticosteroids (P = 0.02 for interaction) and combination treatment (P = 0.01) but not for long-acting anticholinergics (P = 0.46). A limitation of this analysis is its exclusive focus on exacerbations and lack of FEV1 data for individual patients.
Conclusion: We found no evidence that one single inhaled drug regimen is more effective than another in reducing exacerbations. Inhaled corticosteroids when added to long-acting beta-agonists reduce exacerbations only in patients with COPD with FEV1 </= 40%.
Figures


References
-
- Lopez AD, Shibuya K, Rao C, Mathers CD, Hansell AL, Held LS, Schmid V, Buist S. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27:397–412. - PubMed
-
- Yang IA, Fong KM, Sim EH, Black PN, Lasserson TJ. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2007;2:CD002991. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
